My approach to revision has always been to attempt a question, then when I fail use it as a 'spring board' to bounce off into a topic that the question has highlighted I'm less familiar with. What I've always found in the past is that initially each question produces a whole set of 'learning needs', but as revision progresses fewer 'black holes of knowledge' or 'grey holes of partially forgotten information' are revealed.
It was therefore not entirely a surprise that the first time I sat down to revise I only got through one question as it uncovered so many things I needed to read up on!
These were:
- pituitary apoplexy (which in turn prompted revision of the anatomy of the cavernous sinus)
- analysis of
CSF fluid
- brief review of
Addisons disease
As you can see, there is a certain degree of randomness about the topics generated each day. To try and make this blog easier for me (and potentially others) to use for revision in the future I've decided to split each day into a series of 'mini-battles', essentially separating the topics into different posts. So, in the case of today this post is battle 1.1 and will just cover pituitary apoplexy, and then I'll do a post entitled battle 1.2 to cover analysis of CSF fluid and battle 1.3 to cover Addissons disease.
The other benefit to this is that if you want to avoid my waffle you can just skim down the first part of each post headed by 'battle x.1' and then all other battles will be info-dense, waffle light but hopefully still contain a sprinkling of humour!
So, with no further ado onto to the main meat of battle 1.1!
Pituitary apoplexy
Pituitary apoplexy describes a condition caused by sudden haemorrhage into or infarction of the pituitary gland, usually in a patient already known to have a pituitary adenoma.
It should be considered in questions where the patient has meningitis-like symptoms (neck stiffness, headache, vomiting) and also eye signs such as bitemporal superior quadrantanopia or opthalmoplegia. Low BP may also be a feature.
Pituitary apoplexy is diagnosed by CT/MRI, and treatment is essentially surgical but immediate medical management would involve ABCD, balancing of electrolyte disturbances and a dose of hydrocortisone, since loss of the pituitary is going to cause levels to plummet (and hence the low BP).
I have a guilty love of eponymous syndromes and happily pituitary apoplexy has one associated with it: Sheehans syndrome. To highlight any eponymous syndromes snuck into posts I will be writing them in purple...
Sheehans syndrome is pituitary apoplexy after childbirth, usually (but not always) associated with postpartum haemorrhage.
Having revised pituitary apoplexy, it makes sense to just sneak in a spot of relevant anatomy revision (partly cos I'm a geek, partly because if you understand the anatomy it makes the medicine easier):
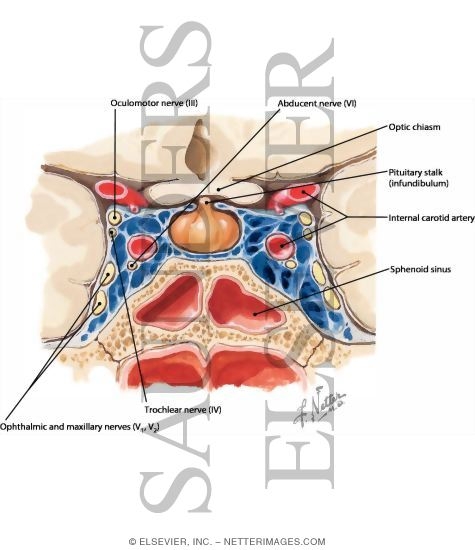
Revision of anatomy of cavernous sinus
The cavernous sinus around the pituitary gland contains CN III, IV, V1, V2 and VI, also the internal carotid artery. Note CN II runs just above it.
A nice picture can be found
here from the fabulous Netter images collection.
Click here for battle 1.2!
{kind=link}