Myeloid cells are essentially all blood cells that are not leukocytes.
It is the commonest leukaemia in adults.
Presentation may be by:
- complications of marrow failure
- anaemia
- infection
- bleeding
- evidence of marrow infiltration
- hepato/splenomegaly
- gum hypertrophy
Diagnosis is by bone marrow biopsy.
Immunophenotyping/cytogenetic analysis is important to guide treatment and indicate prognosis.
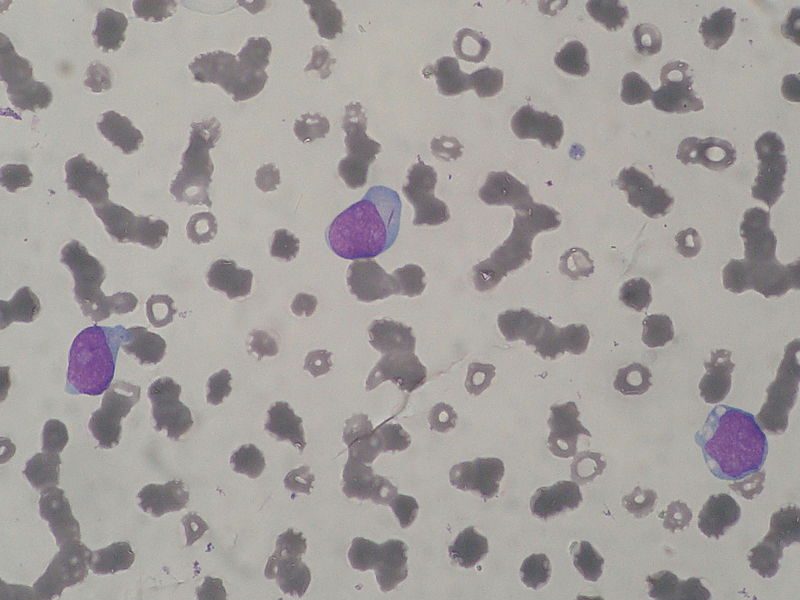
The key feature on microsopy is the auer rod - note the small rod in the cytoplasm of the central cell:
Classification was traditionally done by the FAB (French-American-British) classification, which ran from M0 to M7. The important random facts I remember from this is that M2 is associated with t(8;21) and M3 (aka acute promyelocytic leukaemia, the topic of the next battle) is associated with t(15;17). Both of these translocations are associated with a good prognosis.
Now the WHO classification is more commonly used. It is rather complex and includes catagories such as 'AML with characteristic abnormalities' and 'AML therapy-related' If you are interested the further reading link at the bottom will tell you more.
Treatment is supportive care and intensive chemotherapy, usually with cytosine arabinoside and daunorubicin, or bone marrow transplant.
Survival with no treatment is around 2 months; with chemo there is around 20% 3 yr survival.
For the really keen:
Now lets briefly look at acute promyelocytic leukaemia...