MRCP revision battle 38.1: Von Willebrands Disease
MRCP revision battle 38.2: B cell disorders
MRCP revision battle 38.3: T cell disorders
MRCP revision battle 38.4: Combined B and T cell disorders
MRCP revision battle 38.5: Thrombotic thrombocytopenic purpura
MRCP revision battle 38.6: Microangiopathic haemolytic anaemia
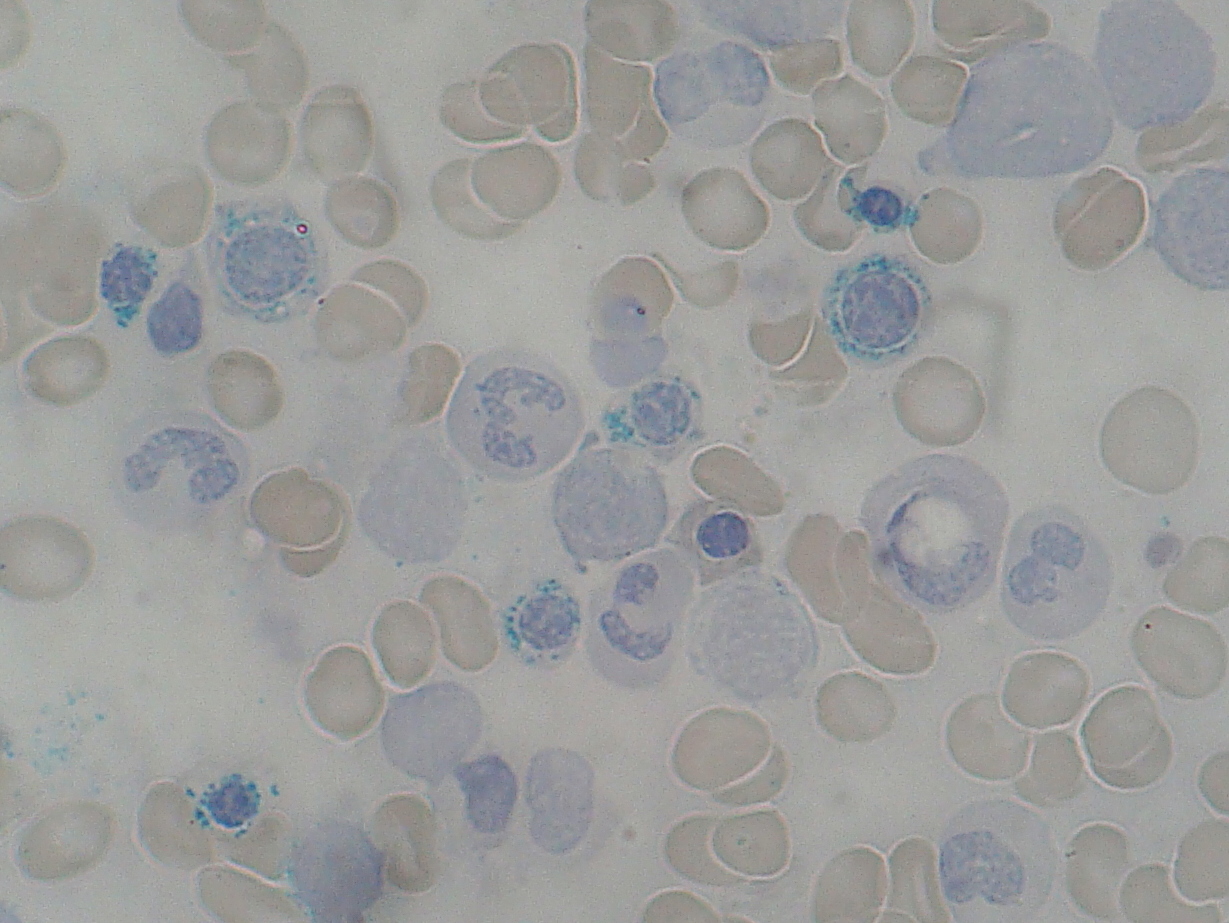
MRCP revision battle 38.7: Sideroblastic anaemia
MRCP revision battle 38.1: Von Willebrands Disease
Von Willebrand's disease is the commonest inherited coagulopathy in the UK.
Von Willebrand's factor is a substance made in epithelial cells which:
- helps platelets bind to the exposed subendothelium
- helps platelets bind to each other
- binds to factor VIII, helping prevent its destruction in the circulation
There are many types of Von Willebrand's disease. The commonest 3 are:
- Type 1: decrease in Von Willebrand's factor
- accounts for 80% of Von Willebrand Disease
- autosomal dominant
- Type 2: abnormal form of Von Willebrand's factor
- autosomal dominant
- Type 3: total lack of Von Willebrand's factor
- autosomal recessive
Symptoms/signs of Von Willebrand's disease include bruising, menorrhagia, epistaxis and increased bleeding after tooth extraction (a favourite in MRCP exams)
Diagnosis is by:
- low levels factor VIII
- low levels VWF antigen
- deficient ristocetin-induced platelet aggregation
Treatment is:
- DDVAP (=desmopressin) in mild disease
- factor VIII concentrate/cryoprecipitate in severe disease
- avoid NSAIDs.
Next up.... B cell disorders