It accounts for 5-10% of all strokes.
Causes:
- ruptured berry aneurysm (80%)
- malformations (15%)
- post trauma
Common sites of berry aneurysms are:
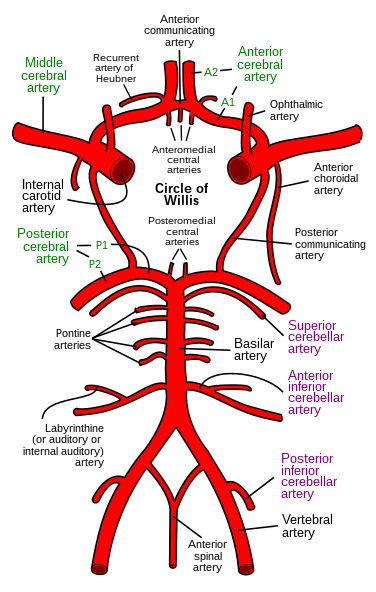
- junction of the posterior communicating artery with the internal carotid
- junction of the anterior communicating artery with the anterior cerebral artery
- the bifurcation of the middle cerebral artery
If (like me) your anatomy of the circle of willis is a little rusty the wiki commons image below might help refresh your memory:
15% of berry aneurysms are multiple.
Subarachnoid haemorrhages are associated with:
- polycystic kidneys
- coarctation of the aorta
- Ehlers-Danlos syndrome
- PAN
Classical presentation is a thunderclap occipital headache "as if kicked in head" with vomiting and neck stiffness.
Around 6% of patients will have had a sentinel headache before.
Investigation is:
- CT - >90% of bleeds detected
- LP - done >12hrs after onset looking for xanthochromia
Management:
- neurosurgical referral
- prompt angiography if surgery likely
- nimodipine
On to another neuro topic - normal pressure hydrocephalus