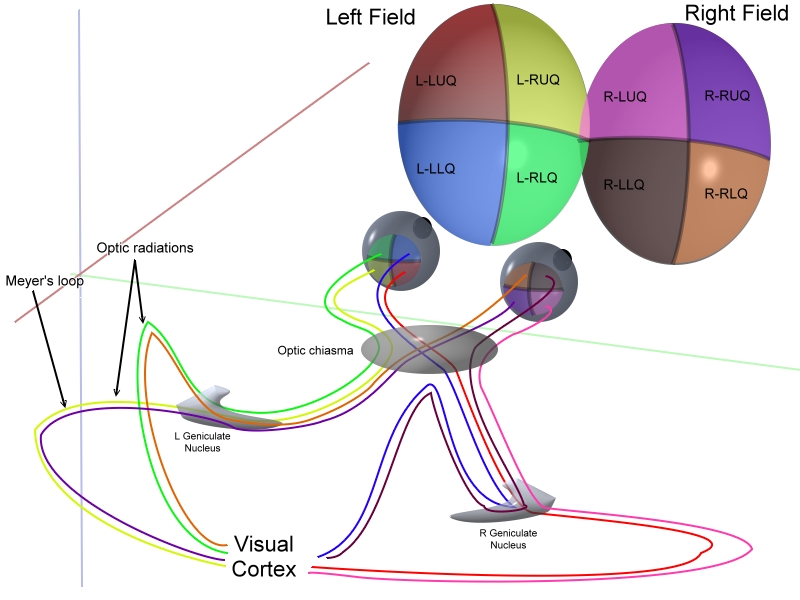
The basic anatomy is illustrated below:
Armed this this anatomy lets look at the various patterns of field defect...
1: Bitemporal hemianopia

- caused by compression of the optic chiasm
- upper affected more than lower = due to pituitary tumour
- lower affected more than upper = due to craniopharyngioma
- I personally remember this as UP London City
2: Homonymous quadrantanopia

- superior homonymous quadrantanopia is a lesion in the temporal lobe
- inferior homonymous quadrantanopia is a lesion in the parietal lobe
- this can be remembered by thinking PITS - parietal inferior temporal superior
- if the defect is incongruous it is in the optic tract
- if the defect is congruous it is in the optic radiation/cortex
3: Homonymous hemianopia

- injury to the brain (eg bleed, tumour) on the opposite side to the field defect
4: Central scotoma

- usually caused by optic neuritis
5: Binasal hemianopia

- rare
- ?calcification of carotids
Note that the fovea is supplied by both the PCA and MCA so may be spared in a PCA CVA.
In the calcarine sulcus peripheral regions are processed anteriorly while central regions are processed posteriorly.
Finally remember cortical blindness:
- caused by bilateral occipital infarcts
- pupillary responses are preserved
- possibly small macular sparing
- patient may deny they have vision loss (=Anton's syndrome)
Wow, that was lots for one battle... lets move on to some urine for light relief...