Insulinoma is the commonest pancreatic endocrine tumour.
10% are malignant, 10% are multiple.
If multiple, 50% are associated with MEN-1.
Presentation tends to be with the symptoms of hypoglycaemia (revise battle 29.1 if you need to be reminded of these)
Diagnosis is by supervised prolonged fasting.
Treatment is surgical excision.
Onwards for a quick tour of metabolic syndrome...
Thursday, 28 October 2010
MRCP revision battle 36.6: Metabolic syndrome
Metabolic syndrome (AKA syndrome X) is a combination of disorders that increase a patient's risk of cardiovascular disease/diabetes.
It is defined as:
Metabolic syndrome is associated with:
Now for the final battle of the day, phaeochromocytoma...
It is defined as:
- central obesity (= waist >94cm in europeans) OR BMI >30
- PLUS 2 of the following 4:
- triglycerides >1.7
- low HDL
- BP >130/85
- fasting glucose >5.6 or type 2 DM
Metabolic syndrome is associated with:
- raised uric acid levels
- non-alcoholic fatty liver
- PCOS
Now for the final battle of the day, phaeochromocytoma...
MRCP revision battle 36.7: Phaeochromocytoma
Phaeochromocytomas are rare, catecholamine (=adrenaline, noradrenaline, dopamine ) producing tumours.
Presentations are variable and can include:
The triad of headache, sweating and palpitations is 90% predictive.
Lots of facts to remember about phaeochromocytomas follow the rule of 10%:
10% are familial (= MEN II, neurofibrosis, Von Hippel Lindau)
10% are bilateral, 10% are malignant and10% are extraadrenal
The commonest extraadrenal site is the organ of Zuckerkandl, which is adjacent to the bifurcation of the aorta.
Diagnosis is by VMA in urine and CT/MRI (show up bright white on T2 weighted MRI)
Treatment is surgery with pre-op alpha and beta blockade (alpha blocker of choice = phenoxybenzamine)
Recurrence is possible so these patients should be followed up lifelong.
Thats all for today, hopefully more tomorrow!
Presentations are variable and can include:
- headaches
- visual disturbances
- chest tightness
- palpitations
- hypertension (70% persistent, 30% episodic)
- hypotension/postural hypotension is also possible
- faints
- abdominal pain
The triad of headache, sweating and palpitations is 90% predictive.
Lots of facts to remember about phaeochromocytomas follow the rule of 10%:
10% are familial (= MEN II, neurofibrosis, Von Hippel Lindau)
10% are bilateral, 10% are malignant and10% are extraadrenal
The commonest extraadrenal site is the organ of Zuckerkandl, which is adjacent to the bifurcation of the aorta.
Diagnosis is by VMA in urine and CT/MRI (show up bright white on T2 weighted MRI)
Treatment is surgery with pre-op alpha and beta blockade (alpha blocker of choice = phenoxybenzamine)
Recurrence is possible so these patients should be followed up lifelong.
Thats all for today, hopefully more tomorrow!
Tuesday, 26 October 2010
MRCP revision battle 35.1: Graves' disease
Today is going to be a bit of a thyroid binge with a little gap to end on...
MRCP revision battle 35.1: Graves' disease
MRCP revision battle 35.2: Subacute (de Quervain's) thyroiditis
MRCP revision battle 35.3: Hashimoto's thyroiditis
MRCP revision battle 35.4: Drugs causing hypothyoidism
MRCP revision battle 35.5: Thyroid storm
MRCP revision battle 35.6: Anion gap
MRCP revision battle 35.1: Graves' disease
Graves' disease is an autoimmune condition which causes hyperthyroidism. Autoantibodies against the thyroid gland are present. This may be antithyroid peroxidase antibodies or antithyroglobulin antibodies (neither are specific as they may also found in Hashimotos) or TSH receptor antibody (specific)
Features of Graves' disease include:
Associated with Graves' disease include:
Treatment options for Graves are:
on to battle 35.2...
MRCP revision battle 35.1: Graves' disease
MRCP revision battle 35.2: Subacute (de Quervain's) thyroiditis
MRCP revision battle 35.3: Hashimoto's thyroiditis
MRCP revision battle 35.4: Drugs causing hypothyoidism
MRCP revision battle 35.5: Thyroid storm
MRCP revision battle 35.6: Anion gap
MRCP revision battle 35.1: Graves' disease
Graves' disease is an autoimmune condition which causes hyperthyroidism. Autoantibodies against the thyroid gland are present. This may be antithyroid peroxidase antibodies or antithyroglobulin antibodies (neither are specific as they may also found in Hashimotos) or TSH receptor antibody (specific)
Features of Graves' disease include:
- eye disease (see revision battle 29.2 to recap which features are Graves' disease specific)
- pretibial myxoedema - only found in Graves
- thyroid acropachy = clubbing, painful toe and finger swelling - also only in Graves
- diffuse thyroid enlargement
Associated with Graves' disease include:
- diabetes
- vitiligo
- Addisons
Treatment options for Graves are:
- titrate antithyroid drugs
- start at 40mg carbimazole
- continue for 12-18 months
- less side effects
- block and replace
- start at 40mg carbimazole, levothyroxine once euthyroid
- treat for 6 to 9 months
- more side effects
- radioiodine
on to battle 35.2...
MRCP revision battle 35.2: Subacute (de Quervain's) thyroiditis
Subacute (de Quervain's) thyroiditis is the label given to a viral infection which causes a painful goitre and potentially transient hyper or hypo thyroidism.
In addition to a painful goitre the patient may have a fever and dysphagia.
Classically it occurs following a upper respiratory tract infection but it may occur after any viral illness (mumps, adenovirus) and also post-partum.
Histology would show multi-nucleated giant cells.
Radioiodine uptake is typically less than 1% at 24 hrs.
Treatment is with NSAIDs. It resolves spontaneously.
Onwards to Hashimotos...
In addition to a painful goitre the patient may have a fever and dysphagia.
Classically it occurs following a upper respiratory tract infection but it may occur after any viral illness (mumps, adenovirus) and also post-partum.
Histology would show multi-nucleated giant cells.
Radioiodine uptake is typically less than 1% at 24 hrs.
Treatment is with NSAIDs. It resolves spontaneously.
Onwards to Hashimotos...
MRCP revision battle 35.3: Hashimoto's thyroiditis
Hashimoto's thyroiditis is an autoimmune condition causing hypothyroidism.
It is associated with high titres of antithyroid peroxidase antibodies or antithyroglobulin antibodies (neither are specific as they may also found in Graves' disease)
Patients with Hashimotos have a goitre due to lymphocytic and plasma cell infiltration. The gotire is firm and non-tender.
Clinically patients' with Hashimotos may be hypothyroid, euthyroid or occasionally initially even hyperthyroid!
So lets move away from this autoimmune cause of hypothyroidism to look at drugs causing hypothyroidism...
It is associated with high titres of antithyroid peroxidase antibodies or antithyroglobulin antibodies (neither are specific as they may also found in Graves' disease)
Patients with Hashimotos have a goitre due to lymphocytic and plasma cell infiltration. The gotire is firm and non-tender.
Clinically patients' with Hashimotos may be hypothyroid, euthyroid or occasionally initially even hyperthyroid!
So lets move away from this autoimmune cause of hypothyroidism to look at drugs causing hypothyroidism...
MRCP revision battle 35.4: Drugs causing hypothyoidism
Drugs which can cause hypothyroidism include:
On to the final bit of thyroid for the day: thyroid storm
- lithium
- interferon
- amiodarone
- phenytoin
- aspirin
- oestrogens
- furosemide
On to the final bit of thyroid for the day: thyroid storm
MRCP revision battle 35.5: Thyroid storm
Thyroid storms may be precipitated by:
Iatrogenic thyroxine excess doesn't usually cause a storm.
Features of a thyroid storm include:
Treatment:
Thats the end of the thyroid binge - now to 'mind the gap..'
- recent thyroid surgery
- radioiodine
- infection
- MI
- trauma
Iatrogenic thyroxine excess doesn't usually cause a storm.
Features of a thyroid storm include:
- fever >38.5C
- tachycardia
- confusion
- nausea and vomiting
- hypertension
- heart failure
Treatment:
- treat precipitating event
- propranolol
- antithyroid drugs eg propylthiouracil or carbimazole
- dexamethasone/hydrocortisone - blocks T4 to T3
- Lugol's solution
- ?digoxin to slow heart.
Thats the end of the thyroid binge - now to 'mind the gap..'
MRCP revision battle 35.6: Anion gap
If you have a patient with metabolic acidosis you need to calculate their anion gap. This is very simple to do, so long as you can remember the following formula (which unfortunately I never can):
A 'normal' anion gap is 10 to 18mmol/l (which can be recalled as roughly the ages you attend secondary school for)
Causes of a raised anion gap may be recalled as LUKES:
A more comprehensive list can be recalled by 'cute dimples' = cyanide, urate, toulene, ethylene glycol, diabetic ketoacidosis, isoniazid, methanol, propylene glycol, lactic acid, salicylates
Causes of a metabolic acidosis with a normal anion gap can be recalled as FUSEDCARS:
Hopefully thats demystified the anion gap for you.
Anion gap = (Na + K) - (Cl + HCO3)
A 'normal' anion gap is 10 to 18mmol/l (which can be recalled as roughly the ages you attend secondary school for)
Causes of a raised anion gap may be recalled as LUKES:
- lactic acid (shock, infection, hypoxia)
- urate (renal failure)
- ketones (diabetes, alcohol)
- ethylene glycol/methanol
- salicylate
A more comprehensive list can be recalled by 'cute dimples' = cyanide, urate, toulene, ethylene glycol, diabetic ketoacidosis, isoniazid, methanol, propylene glycol, lactic acid, salicylates
Causes of a metabolic acidosis with a normal anion gap can be recalled as FUSEDCARS:
- fistula (pancreatic)
- uretogastric conduits
- saline administration
- endocrine (hyperparathyroidism)
- diarrhoea
- carbonic anhydrase inhibitors (acetazolamide)
- ammonium chloride
- renal tubular acidosis
- spironolactone
Hopefully thats demystified the anion gap for you.
Monday, 25 October 2010
MRCP revision battle 34.1: The first heart sound
I've just had a whole week off revising. Very bad from a passing MRCP point of view. Very good from a remaining sane, keeping friends and staying up-to-date with all the other bits of paper medicine in the UK requires. Since the exam is now under a month away however I'd better buckle down to it...
MRCP revision battle 34.1: The first heart sound
MRCP revision battle 34.2: The second heart sound
MRCP revision battle 34.3: The third and fourth heart sounds
MRCP revision battle 34.4: Sodium Valproate
MRCP revision battle 34.5: Salicylate overdose
MRCP revision battle 34.6: Haemodialysis in overdose
MRCP revision battle 34.7: Cyanide poisoning
MRCP revision battle 34.8: Phentolamine
MRCP revision battle 34.1: The first heart sound
The first heart sound is made by the closure of the mitral and tricuspid valves.
A loud S1 may be due to:
A soft S1 may be due to:
A s p l i t S1 is caused by:
A variable S1 is caused by:
On to the second heart sound....
MRCP revision battle 34.1: The first heart sound
MRCP revision battle 34.2: The second heart sound
MRCP revision battle 34.3: The third and fourth heart sounds
MRCP revision battle 34.4: Sodium Valproate
MRCP revision battle 34.5: Salicylate overdose
MRCP revision battle 34.6: Haemodialysis in overdose
MRCP revision battle 34.7: Cyanide poisoning
MRCP revision battle 34.8: Phentolamine
MRCP revision battle 34.1: The first heart sound
The first heart sound is made by the closure of the mitral and tricuspid valves.
A loud S1 may be due to:
- mitral stenosis
- hyperdynamic states
- short PR
A soft S1 may be due to:
- long PR
- mitral regurgitation
A s p l i t S1 is caused by:
- RBBB
- LBBB
- VT
- inspiration
- Ebsteins abnormality
A variable S1 is caused by:
- complete heart block
- AF
On to the second heart sound....
MRCP revision battle 34.2: The second heart sound
The second heart sound comprises of the closure of the aortic and pulmonary valves.They usually close <0.05secs apart and in alphabetical order, with the aortic valve closing first.
A loud S2 may be due to:
A soft S2 may be due to aortic stenosis.
A w i d e l y s p l i t second heart sound occurs in:
A reverse split (=paradoxical split) second heart sound occurs in:
Onwards for the third and fourth heart sounds...
A loud S2 may be due to:
- systemic hypertension (=loud A2)
- pulmonary hypertension (=loud P2)
- tachycardia
A soft S2 may be due to aortic stenosis.
A w i d e l y s p l i t second heart sound occurs in:
- RBBB
- deep inspiration
- mitral regurgitation
- pulmonary stenosis
A reverse split (=paradoxical split) second heart sound occurs in:
- LBBB
- severe aortic stenosis
- right ventricular pacing
- WPW type 2
- patent ductus arteriosus
Onwards for the third and fourth heart sounds...
MRCP revision battle 34.3: The third and fourth heart sounds
Third heart sound
Third heart sound, AKA gallop rhythm, can be perfectly normal in children and young adults.
It is due to passive filling of the ventricles when the atrioventricular valves open.
In the over 40s it is pathological and may indicate:
S1 S2 S3
The sound of the 3rd heart sound may be remembered as 'Kentucky' or 'SLOSH-ing in'
Fourth heart sound
A 4th heart sound is caused by atrial contraction against stiff ventricles.
It occurs in:
S4 S1 S2
It can be remembered as 'Tennessee' or 'a STIFF wall'
I thoroughly recommend this website to listen to them http://www.wilkes.med.ucla.edu/Rubintro.htm
Now away from cardiology and to a bit of pharmacology - sodium valproate....
Third heart sound, AKA gallop rhythm, can be perfectly normal in children and young adults.
It is due to passive filling of the ventricles when the atrioventricular valves open.
In the over 40s it is pathological and may indicate:
- mitral regurgitation
- VSD
- CCF
- constrictive pericarditis
S1 S2 S3
The sound of the 3rd heart sound may be remembered as 'Kentucky' or 'SLOSH-ing in'
Fourth heart sound
A 4th heart sound is caused by atrial contraction against stiff ventricles.
It occurs in:
- aortic stenosis
- HOCM
- hypertension
S4 S1 S2
It can be remembered as 'Tennessee' or 'a STIFF wall'
I thoroughly recommend this website to listen to them http://www.wilkes.med.ucla.edu/Rubintro.htm
Now away from cardiology and to a bit of pharmacology - sodium valproate....
MRCP revision battle 34.4: Sodium valproate
Sodium valproate is a drug used in epilepsy.
It is a P450 inhibitor.
It has the highest risk of birth defects of any of the anti-epileptic drugs.
Sodium valproate also has an impressive plethora of unfortunate side effects which often appear in MRCP questions:
As always with long lists of side effects its probable best to try and imprint on your mind a cartoon image of an unfortunate patient who is suffering from all of these side effects. Personally I have a bald man who has big breasts and a fat, pregnant stomach, who is walking along in an ataxic way, covered in bruises (from his thrombocytopenia and crashing into things with his ataxic gait) while also vomiting and pointing with his trembling fingers to his liver and pancreas.
On that pretty image, lets move on to battle 33.5...
It is a P450 inhibitor.
It has the highest risk of birth defects of any of the anti-epileptic drugs.
Sodium valproate also has an impressive plethora of unfortunate side effects which often appear in MRCP questions:
- alopecia
- nausea
- gynaecomastia
- weight gain
- tremor
- hepatitis
- pancreatitis
- tetratrogenic
- ataxia
- thrombocytopenia
As always with long lists of side effects its probable best to try and imprint on your mind a cartoon image of an unfortunate patient who is suffering from all of these side effects. Personally I have a bald man who has big breasts and a fat, pregnant stomach, who is walking along in an ataxic way, covered in bruises (from his thrombocytopenia and crashing into things with his ataxic gait) while also vomiting and pointing with his trembling fingers to his liver and pancreas.
On that pretty image, lets move on to battle 33.5...
MRCP revision battle 34.5: Salicylate overdose
Patients who have taken a salicylate overdose are potentially more interesting than those who have taken a paracetamol overdose as salicylate poisoning actually has early clinical features you can look out for, such as:
A blood gas should show a mixed respiratory alkalosis and metabolic acidosis, and potentially a low potassium.
The sweating and pyrexia are due to uncoupling of oxidative phosphorylation.
The effects of salicylate are dose related:
Later features of salicylate poisoning include:
Treatment:
Lets move on to consider use of haemodialysis in overdoses in general...
- sweating
- tinnitus
- dizziness
- pyrexia
- hyperventilation
A blood gas should show a mixed respiratory alkalosis and metabolic acidosis, and potentially a low potassium.
The sweating and pyrexia are due to uncoupling of oxidative phosphorylation.
The effects of salicylate are dose related:
- 150mg/kg: mild
- 250mg/kg: moderate
- >500mg/kg: severe
Later features of salicylate poisoning include:
- renal failure
- hypo or hyperglycaemia
- seizures
- acidosis
Treatment:
- activated charcoal if within 1 hr
- correct acidosis with 1.26% sodium bicarb
- haemodialysis if:
- conc >700mg/l
- metabolic acidosis resistant to treatment
- acute renal failure
- pulmonary oedema
- seizures
- urinary alkalinization is rarely used and is contra-indicated in cerebral or pulmonary oedema
Lets move on to consider use of haemodialysis in overdoses in general...
MRCP revision battle 34.6: Haemodialysis in overdose
Haemodialysis is not helpful in removing a drug if:
The drugs that are appropriate for haemodialysis can be remembered as BLAST:
Charcoal haemoperfusion may be considered for:
Now for a touch of cyanide poisoning....
- the drug has a large volume of distribution (eg amiodarone, paraquat)
- the drug is highly protein-bound (digoxin, phenytoin)
The drugs that are appropriate for haemodialysis can be remembered as BLAST:
- Barbituates
- Lithium
- Alcohol (methanol/ethanol)
- Salicylate
- Theophylline
Charcoal haemoperfusion may be considered for:
- paracetamol
- theophylline
Now for a touch of cyanide poisoning....
MRCP revision battle 34.7: Cyanide poisoning
Cyanide is used in insecticides, photography and found in some metals.
It's toxicity comes from inhibition of oxidising enzymes, which happily is reversible.
The classical features of cyanide poisoning are:
Acute signs of cyanide poisoning include:
Chronic signs of cyanide poisoning include:
Treatment is with 100% oxygen and IV dicolbalt edetate
Onwards for a very brief final battle of the day: phentolamine
It's toxicity comes from inhibition of oxidising enzymes, which happily is reversible.
The classical features of cyanide poisoning are:
- brick red skin
- smell of bitter almonds
Acute signs of cyanide poisoning include:
- hypotension
- hypoxia
- headache
- confusion
Chronic signs of cyanide poisoning include:
- ataxia
- peripheral neuropathy
- dermatitis
Treatment is with 100% oxygen and IV dicolbalt edetate
Onwards for a very brief final battle of the day: phentolamine
MRCP revision battle 34.8: Phentolamine
Phentolamine is a non-selective alpha-antagonist.
Its main action is vasodilation due to alpha-1 blockade.
In the context of MRCP the most important snippet to remember is that phentolamine is used to treat adrenaline-induced ischaemia (eg idiot houseofficer uses lidocaine with adrenaline in ring block, what ya gonna do? or clumsy dentist stabs little finger with his anaesthetic needle and its going blue, how will you treat it?)
In a broader context it can also be helpful in hypertension due to phaeochromocytoma or cocaine.
Thats all for today, more tomorrow!
Its main action is vasodilation due to alpha-1 blockade.
In the context of MRCP the most important snippet to remember is that phentolamine is used to treat adrenaline-induced ischaemia (eg idiot houseofficer uses lidocaine with adrenaline in ring block, what ya gonna do? or clumsy dentist stabs little finger with his anaesthetic needle and its going blue, how will you treat it?)
In a broader context it can also be helpful in hypertension due to phaeochromocytoma or cocaine.
Thats all for today, more tomorrow!
Monday, 18 October 2010
MRCP revision battle 33.1: Myeloma
So today is going to be a galavant through the world of paraproteinaemias, taking in 4 of the top 6 causes (myeloma, Waldenstrom's, MGUS and amyloid; lymphoma/leukaemia related are not discussed, nor is heavy chain disease)
While on the topic of paraproteinaemia is seems appropriate to cover hyperviscosity syndrome, which lends itself to a quick forray into polycythaemia and then on to two completely random topics to round off the day.
Enjoy!
MRCP revision battle 33.1: Myeloma
MRCP revision battle 33.2: Hyperviscosity syndrome
MRCP revision battle 33.3: Waldenstrom's macroglobulinaemia
MRCP revision battle 33.4: MGUS
MRCP revision battle 33.5: Amyloidosis
MRCP revision battle 33.6: Polycythaemia
MRCP revision battle 33.7: Levels of evidence
MRCP revision battle 33.8: Holmes Adie pupil
MRCP revision battle 33.1: Myeloma
Myeloma is a malignant monoclonal proliferation of plasma cells.
The commonest subclass is IgG (IgG>IgA>IgM)
Symptoms:
Investigations:
The diagnostic criteria for myeloma is:
Treatment:
Complications of myeloma include:
Survival with myeloma tends to be 3-4 yrs.
Higher beta 2 microglobulin implies a worse prognosis.
Onwards for a bit more about hyperviscosity syndrome....
While on the topic of paraproteinaemia is seems appropriate to cover hyperviscosity syndrome, which lends itself to a quick forray into polycythaemia and then on to two completely random topics to round off the day.
Enjoy!
MRCP revision battle 33.1: Myeloma
MRCP revision battle 33.2: Hyperviscosity syndrome
MRCP revision battle 33.3: Waldenstrom's macroglobulinaemia
MRCP revision battle 33.4: MGUS
MRCP revision battle 33.5: Amyloidosis
MRCP revision battle 33.6: Polycythaemia
MRCP revision battle 33.7: Levels of evidence
MRCP revision battle 33.8: Holmes Adie pupil
MRCP revision battle 33.1: Myeloma
Myeloma is a malignant monoclonal proliferation of plasma cells.
The commonest subclass is IgG (IgG>IgA>IgM)
Symptoms:
- osteolytic bone lesions --> backache/pathological fractures
- symptoms of hypercalcaemia
- bacterial infections due to immunoparesis
- renal impairment due to light chains
Investigations:
- Bloods:
- normocytic normochromic anaemia
- rouleaux on blood film
- raised calcium (40%)
- raised urea and creatinine
- raised ESR
- Urine
- Bence Jones proteins (=free serum light chains) in urine (66%)
- XR
- ?pepper pot skull, vertebral collapse
The diagnostic criteria for myeloma is:
- monoclonal protein band in serum or urine electrophoresis
- increased plasma cells on BM biopsy
- evidence of end organ damage from myeloma
Treatment:
- supportive
- chemo
- younger patients: aggressive (VAD - vincristine, adriamycin, dexamethasone)
- older patients: less aggressive (CDT - cyclophosphamide, dexamethasone, thalidomide)
Complications of myeloma include:
- Hyperviscosity syndrome
- Hyperviscosity syndrome occurs most commonly in IgM myeloma (IgM>IgA>IgG)
- Transfusions should be avoided in hyperviscosity syndrome.
- hypercalcaemia
- spinal cord compression
- acute renal failure
- AL amyloidosis (15%)
Survival with myeloma tends to be 3-4 yrs.
Higher beta 2 microglobulin implies a worse prognosis.
Onwards for a bit more about hyperviscosity syndrome....
MRCP revision battle 33.2: Hyperviscosity syndrome
Hyperviscosity syndrome is a condition in which the viscosity (='stickiness') of the blood has increased to a degree which prevents easy flow through the microcirculation.
This causes symptoms such as:
The visual disturbance is described as 'looking through a watery car windscreen'
The optic disc may occur blurred.
Normal plasma viscosity is 1.4-1.8. Hyperviscosity syndrome develops above around 4.
Causes of hyperviscosity syndrome include:
Treatment depends on the cause; in myeloma/waldenstroms the patient needs plasmaphersis whereas in polycythaemia the treatment is venesection.
So now seems a good time to battle Waldenstrom's macroglobulinaemia...
This causes symptoms such as:
- lethargy
- confusion
- headache
- visual disturbances
- spontaneous bleeding
The visual disturbance is described as 'looking through a watery car windscreen'
The optic disc may occur blurred.
Normal plasma viscosity is 1.4-1.8. Hyperviscosity syndrome develops above around 4.
Causes of hyperviscosity syndrome include:
- myeloma
- Waldenstroms macroglobulinaemia
- leukaemias
- polycythaemia
Treatment depends on the cause; in myeloma/waldenstroms the patient needs plasmaphersis whereas in polycythaemia the treatment is venesection.
So now seems a good time to battle Waldenstrom's macroglobulinaemia...
MRCP revision battle 33.3: Waldenstrom's macroglobulinaemia
Waldenstrom's macroglobulinaemia, AKA lymphoplasmacytoid lymphoma, is a condition in which monoclonal proliferation of terminally differentiated lymphocytes results in a monoclonal IgM paraprotein.
The significance of this is that IgM carries a high risk of hyperviscosity syndrome.
Treatment for Waldenstom's:
On to another paraproteinaemia, MGUS...
The significance of this is that IgM carries a high risk of hyperviscosity syndrome.
Treatment for Waldenstom's:
- none if asymptomatic
- plasmapheresis if hyperviscosity
- ? chemo
On to another paraproteinaemia, MGUS...
MRCP revision battle 33.4: MGUS
MGUS stands for monoclonal gammopathy of undetermined significance.
As the name suggests, it is a low-level paraproteinaemia of unknown relevance.
It is common, affecting around 3% of those over 70 yrs of age.
For MGUS to be diagnosed the following diagnostic criteria must be met:
Around 10% have myeloma at 5yrs so management tends to be yearly observation.
On to amyloidosis...
As the name suggests, it is a low-level paraproteinaemia of unknown relevance.
It is common, affecting around 3% of those over 70 yrs of age.
For MGUS to be diagnosed the following diagnostic criteria must be met:
- low level paraprotein (<30g/l)
- less than 10% plasma cells on BM
- no clinical evidence of myeloma.
Around 10% have myeloma at 5yrs so management tends to be yearly observation.
On to amyloidosis...
MRCP revision battle 33.6: Polycythaemia
Polycythaemia is a raised red cell count and haemocrit, defined as >0.52 in males or >0.48 in females.
The first thing to establish is if the polycythaemis is 'true/absolute' or 'relative/pseudo'.
Relative/pseudo polycythaemia occurs due to decreased plasma volume. This may occur due to dehydration (eg vomiting, diarrhoea, diuretics)
A special form of relative polycythaemia is Gaisbocks. This tends to affect middle-aged men and is attributed to stress (hypertension, smoking, mild obesity) causing a chronically reduced plasma volume.
True/absolute polycythaemis is due to raised red cell mass.
It can be further divided into primary true polycythaemia and secondary true polycythaemia.
Primary true polycythaemia = polycythaemia rubra vera
Polycythaemia rubra vera is associated with JAK2 mutation in 95% of cases.
It peaks in the 6th decade.
Features include:
WCC/platelets/neutrophil alkaline phosphatase are raised; this helps distinguish primary from secondary polycythaemia.
Secondary polycythaemia
Secondary polycythaemia is due to raised erythropoietin.
Causes:
Management of true polycthaemia is:
Now for something completely different - levels of evidence...
The first thing to establish is if the polycythaemis is 'true/absolute' or 'relative/pseudo'.
Relative/pseudo polycythaemia occurs due to decreased plasma volume. This may occur due to dehydration (eg vomiting, diarrhoea, diuretics)
A special form of relative polycythaemia is Gaisbocks. This tends to affect middle-aged men and is attributed to stress (hypertension, smoking, mild obesity) causing a chronically reduced plasma volume.
True/absolute polycythaemis is due to raised red cell mass.
It can be further divided into primary true polycythaemia and secondary true polycythaemia.
Primary true polycythaemia = polycythaemia rubra vera
Polycythaemia rubra vera is associated with JAK2 mutation in 95% of cases.
It peaks in the 6th decade.
Features include:
- hyperviscosity-syndrome symptoms
- pruritis, especially after a hot bath
- splenomegaly
- plethoric features
- hypertension in 1/3
- haemorrhage secondary to abnormal platelets
- DVTs/arterial thrombosis
- peptic ulceration
- gout
WCC/platelets/neutrophil alkaline phosphatase are raised; this helps distinguish primary from secondary polycythaemia.
Secondary polycythaemia
Secondary polycythaemia is due to raised erythropoietin.
Causes:
- physiological - neonates, high altitude
- congenital cyanotic heart disease
- smoking/COPD
- HbM
- renal cysts
- post renal transplant
- fibroids
- hepatoma
Management of true polycthaemia is:
- venesection
- hydroxyurea to supress erythropoesis
- aspirin
Now for something completely different - levels of evidence...
MRCP revision battle 33.7: Levels of evidence
In this age of evidence-based medicine there is a scale to judge how "good" the evidence is:
Ia: metaanalysis of RCT
Ib: RCT
IIa: controlled trial
IIb: experimental trial
III: case series, case-control studies
IV: 'expert' opinions
Remember these because the odd MRCP question asks you what level of evidence a particular study is providing.
To the final MRCP revision battle of the day...
Ia: metaanalysis of RCT
Ib: RCT
IIa: controlled trial
IIb: experimental trial
III: case series, case-control studies
IV: 'expert' opinions
Remember these because the odd MRCP question asks you what level of evidence a particular study is providing.
To the final MRCP revision battle of the day...
MRCP revision battle 33.8: Holmes Adie pupil
Holmes-Adie pupil is a dilated (myotonic) pupil.
It is a benign condition.
Females (70%) > males (20%)
Unilateral in 80% of cases
A Holmes-Adie pupil is sluggish to accomodate and reacts poorly, if at all, to light.
If a Holmes-Adie pupil is associated with absent leg reflexes it is known as Holmes-Adie Syndrome.
Since that was such a short battle lets just throw in a quick recap of the diferentials for a dilated pupil:
It is a benign condition.
Females (70%) > males (20%)
Unilateral in 80% of cases
A Holmes-Adie pupil is sluggish to accomodate and reacts poorly, if at all, to light.
If a Holmes-Adie pupil is associated with absent leg reflexes it is known as Holmes-Adie Syndrome.
Since that was such a short battle lets just throw in a quick recap of the diferentials for a dilated pupil:
- third nerve palsy
- drugs
- antidepressants
- amphetamines
- atropine
- tropicamide
- Holmes-Adie
- trauma - sphincter pupillae rupture
Sunday, 17 October 2010
MRCP revision battle 32.1: Deafness: Rinnes and Webers
Final day in the hat trick of eyes and neurology battles...
MRCP revision battle 32.1: Deafness: Rinnes and Webers
MRCP revision battle 32.2: Tinnitus
MRCP revision battle 32.3: TIA
MRCP revision battle 32.4: Epilepsy
MRCP revision battle 32.5: Macular degeneration
MRCP revision battle 32.6: Glaucoma
MRCP revision battle 32.7: Autonomic neuropathy
MRCP revision battle 32.1: Deafness: Rinnes and Webers
Hearing loss and Rinne and Weber's tests are MRCP favourites.
Remember there are 2 types of deafness:
Tests are done with a 256- 512 Hz tuning fork
Rinne's test:
Weber's test:
Next up - a spot of tinnitus...
MRCP revision battle 32.1: Deafness: Rinnes and Webers
MRCP revision battle 32.2: Tinnitus
MRCP revision battle 32.3: TIA
MRCP revision battle 32.4: Epilepsy
MRCP revision battle 32.5: Macular degeneration
MRCP revision battle 32.6: Glaucoma
MRCP revision battle 32.7: Autonomic neuropathy
MRCP revision battle 32.1: Deafness: Rinnes and Webers
Hearing loss and Rinne and Weber's tests are MRCP favourites.
Remember there are 2 types of deafness:
- conductive deafness
- ear wax
- otosclerosis
- otitis media
- glue ear
- sensorineural deafness
- acoustic neuroma
- Pagets
- MS
- CVA
- Menieres
- head trauma
- noise exposure
- drugs
- aminoglycosides (gentamycin)
- furosemide
- lead
Tests are done with a 256- 512 Hz tuning fork
Rinne's test:
- hold vibrating tuning fork next to ear meatus, then place on mastoid
- ask which is louder
- air conduction (AC) > bone conduction (BC) = normal, or, if hearing is decreased, suggests sensorineural loss
- BC>AC = conductive deafness = Rinne negative
- Remember as: ALS (like the course) - air loudest: sensorineural.
Weber's test:
- hold vibrating tuning fork on forehead
- ask which side it is heard loudest in
- in sensorineural loss it laterals to the unaffected side
- in conductive loss it laterals to the affected side
- midline if normal, or bilateral sensorineural loss
- Remember as: SUCA - sensorineural unaffected, conductive affected.
Next up - a spot of tinnitus...
MRCP revision battle 32.2: Tinnitus
Tinnitus is ringing/buzzing in ears.
Causes include:
Pulsatile tinnitus may indicate carotid artery stenosis or dissection
Now on to the meatier topic of TIAs...
Causes include:
- eax
- viral infections
- presbyacusis
- head injury
- Menieres
- drugs
- aspirin
- furosemide
- gentamycin
Pulsatile tinnitus may indicate carotid artery stenosis or dissection
Now on to the meatier topic of TIAs...
MRCP revision battle 32.4: Epilepsy
Epilepsy is defined as a recurrent tendency to spontaneous, intermittent, abnormal electrical activity in part of the brain, manifest as seizures (OHCM definition)
Epileptic seizures are subdivided into:
Treatment is usually started after the second seizure. It would be started after the first if any of the following conditions apply:
First line treatment depends on the seizure type:
Remember that both sodium valproate and lamotrigine are associated with Steven Johnson syndrome.
Cannot drive until seizure-free for 1 yr, or 3 yrs of night time only seizures.
HGV drivers need to be off meds and seizure-free for 10 yrs.
If a pt has no seizures for 2 yrs, you may consider stopping meds over 2-3 months.
On to battle 32.5...
Epileptic seizures are subdivided into:
- partial seizures = features come from one part of the brain
- simple partial = consciousness not impaired
- complex partial = consciousness impaired - usually temporal lobe, aura may preceed and automatisms may feature
- generalised seizures = features not localisable to one part of the brain
- absence = petit mal = brief <10 second pauses - 3Hz spikes
- atonic = becomes flaccid
- tonic-clonic - classic stiffening and jerking
- myoclonic
Treatment is usually started after the second seizure. It would be started after the first if any of the following conditions apply:
- neurological deficit
- structural abnormality
- EEG unequivocal
- pt/family/carers keen for treatment
First line treatment depends on the seizure type:
- generalised
- 1st line: sodium valproate
- 2nd line: lamotrigine
- partial
- 1st line: carbamezepine
- 2nd line: sodium valproate
- absence
- sodium valproate or ethosuximide
- note that carbamazepine may worsen absence seizures
Remember that both sodium valproate and lamotrigine are associated with Steven Johnson syndrome.
Cannot drive until seizure-free for 1 yr, or 3 yrs of night time only seizures.
HGV drivers need to be off meds and seizure-free for 10 yrs.
If a pt has no seizures for 2 yrs, you may consider stopping meds over 2-3 months.
On to battle 32.5...
MRCP revision battle 32.3: TIA
TIA (=transient ischaemic attack) = sudden onset of focal CNS phenomena which last <24 hours. Caused by temporary occlusion of part of the cerebral circulation.
Causes of TIAs:
Management depends on the ABCD2 score, which is calculated as shown below:
ABCD2 score of 4 or more, or crescendo TIAs (=2 or more in one week):
ABCD2 score of 3 or below, or symptoms >1 week ago:
After specialist review, usually 75mg aspirin OD and dipyridamol OD for 2 yrs.
If pt is aspirin intolerant, prescribe monotherapy of clopidogrel.
If assessed to be a candidate for carotid endarterectomy, imaging should be performed within 1 week of symptom onset and if carotid stenosis of:
Remember pt must inform DVLA and no driving for 1 month (car) or 1 yr (lorry). This increases to 3 months for car if multiple TIAs.
Of course other risk factors (hypertension, alcohol, smoking, etc etc etc) should also be addressed.
Differentials for TIA may include:
Lets move on to tackle epilepsy...
Causes of TIAs:
- thromboembolism
- chiefly from carotids
- may be from heart - AF, mural thrombus etc)
- hyperviscosity
- myeloma
- polycythaemia
- sickle cells
- very high white cells
Management depends on the ABCD2 score, which is calculated as shown below:
- age >60 : 1 point
- BP greater or equal to 140/90 : 1 point
- clinically:
- unilateral weakness : 2 points
- speech disturbance without weakness : 1 point
- duration
- >60 mins : 2 points
- 10 - 59 mins : 1 point
- diabetes : 1 point
ABCD2 score of 4 or more, or crescendo TIAs (=2 or more in one week):
- specialist review within 24 hrs
- start 300mg aspirin OD
ABCD2 score of 3 or below, or symptoms >1 week ago:
- specialist review within a week
- start 300mg aspirin od
After specialist review, usually 75mg aspirin OD and dipyridamol OD for 2 yrs.
If pt is aspirin intolerant, prescribe monotherapy of clopidogrel.
If assessed to be a candidate for carotid endarterectomy, imaging should be performed within 1 week of symptom onset and if carotid stenosis of:
- 50–99% according to NASCET criteria, or
- 70–99% according to ECST criteria
Remember pt must inform DVLA and no driving for 1 month (car) or 1 yr (lorry). This increases to 3 months for car if multiple TIAs.
Of course other risk factors (hypertension, alcohol, smoking, etc etc etc) should also be addressed.
Differentials for TIA may include:
- migraine
- epilepsy
- hypoglycaemia
- malignant hypertension
- MS
Lets move on to tackle epilepsy...
MRCP revision battle 32.5: Macular degeneration
Macular degeneration is the commonest cause of blindness in the UK.
There are 2 types:
Below is an image of dry macular degeneration showing drusen. To link to an image of wet macular degeneration click here

Risk factors for macular degeneration are:
Treatment - there is no cure:
Keeping on eyes, next up is glaucoma...
There are 2 types:
- dry
- drusen - yellow spots in Bruchs membrane
- wet
- choroidal neovascularisation
- worse prognosis
Below is an image of dry macular degeneration showing drusen. To link to an image of wet macular degeneration click here
Risk factors for macular degeneration are:
- age >60
- female
- smoking
- caucasian
- family history
Treatment - there is no cure:
- high dose beta caratene - but may increase risk of lung cancer in smokers
- vitamin C and E - but vit E may increase risk of heart failure
- zinc
- for wet:
- photocoagulation
- anti VEGF
- Ranibizumab
- photodynamic therapy
Keeping on eyes, next up is glaucoma...
MRCP revision battle 32.6: Glaucoma
Glaucoma is damage to the optic nerve, generally due to increase in intra-ocular pressure.
There are 2 types of glaucoma:
Acute closed angle glaucoma
Acute closed angle glaucoma presents as:
Risk factors for closed angle glaucoma include hypermetropia and pupillary dilation.
Management is:
Open angle glaucoma
This affects 2% of over 40s.
Risk factors include:
Features include:
Treatments include:
Now to our final battle of the day, autonomic neuropathy
There are 2 types of glaucoma:
- acute = closed angle glaucoma
- chronic = open angle glaucoma
Acute closed angle glaucoma
Acute closed angle glaucoma presents as:
- pain
- decreased visual acuity
- worsening of pain with mydriasis
- hard, red eye
- halos around lights
- semi-dilated, non-reactive pupil
- pt systemically unwell
Risk factors for closed angle glaucoma include hypermetropia and pupillary dilation.
Management is:
- urgent opthalmic review
- IV acetazolamide (a carbonic anhydrase inhibitor; decreases aqueous secretions)
- topical pilocarpine (constricts pupil)
Open angle glaucoma
This affects 2% of over 40s.
Risk factors include:
- family history
- black
- myopia
- hypertension
- diabetes
Features include:
- peripheral field loss
- decreased visual acuity
- optic disc cupping
Treatments include:
- eye drops (beta blockers or prostaglandins)
- possibly surgery.
Now to our final battle of the day, autonomic neuropathy
MRCP revision battle 32.7: Autonomic neuropathy
Autonomic neuropathy is characterised by:
Causes:
Treatment is symptomatic; remember fludrocortisone as an option for severe postural hypotension.
On that list-intensive battle lets retire for the day.
- postural hypotension
- erectile dysfunction
- constipation or diarrhoea
- urinary retention
- inability to sweat
- loss of decreased heart rate on deep breathing
- Horners
- Holmes-Adie pupil
Causes:
- endocrine
- diabetes
- infective
- HIV
- syphilis
- leprosy
- autoimmune
- SLE
- other
- GBS
- MSA
- parkinson's disease
- liver/renal failure.
Treatment is symptomatic; remember fludrocortisone as an option for severe postural hypotension.
On that list-intensive battle lets retire for the day.
Saturday, 16 October 2010
MRCP revision battle 31.1: Wernicke's Encephalopathy
Day 2 of 3 for lots of neuro...
MRCP revision battle 31.1: Wernicke's Encephalopathy
MRCP revision battle 31.2: Korsakoff's Syndrome
MRCP revision battle 31.3: Multiple Sclerosis
MRCP revision battle 31.4: Menieres Disease
MRCP revision battle 31.5: CJD
MRCP revision battle 31.6: Herpes Zoster Opthalmicus
MRCP revision battle 31.7: Ramsey Hunt Syndrome
MRCP revision battle 31.1: Wernicke's Encephalopathy
Wernicke's encephalopathy is caused by thiamine (=vitamin B1) deficiency.
The classic triad associated with Wernicke's encephalopathy is:
There may also be hypothermia and hypotension.
Thiamine deficiency may result from:
CT brain may show petichial haemorrhages and a low red cell transketolase blood test could prove thiamine deficiency (rarely performed)
Treatment is parenteral thiamine (pabrinex)
If untreated, 20% of patients will die and 85% will develop Korsakoffs.
Which leads us nicely into revision battle 31.2: Korsakoffs syndrome....
MRCP revision battle 31.1: Wernicke's Encephalopathy
MRCP revision battle 31.2: Korsakoff's Syndrome
MRCP revision battle 31.3: Multiple Sclerosis
MRCP revision battle 31.4: Menieres Disease
MRCP revision battle 31.5: CJD
MRCP revision battle 31.6: Herpes Zoster Opthalmicus
MRCP revision battle 31.7: Ramsey Hunt Syndrome
MRCP revision battle 31.1: Wernicke's Encephalopathy
Wernicke's encephalopathy is caused by thiamine (=vitamin B1) deficiency.
The classic triad associated with Wernicke's encephalopathy is:
- opthalmoplegia
- ataxia
- confusion
There may also be hypothermia and hypotension.
Thiamine deficiency may result from:
- alcoholism
- carcinoma of stomach
- anorexia
- vomiting
CT brain may show petichial haemorrhages and a low red cell transketolase blood test could prove thiamine deficiency (rarely performed)
Treatment is parenteral thiamine (pabrinex)
If untreated, 20% of patients will die and 85% will develop Korsakoffs.
Which leads us nicely into revision battle 31.2: Korsakoffs syndrome....
MRCP revision battle 31.2: Korsakoff's Syndrome
Korsakoff's Syndrome is a condition in which there is an inability to build new memories but preservation of other cognitive functions.
It is a chronic disorder, usually following Wernicke's encephalopathy.
The patient has an inability to consolidate new info, retrograde amnesia, patchy preservation of long term memory, a lack of insight and confabulates (=fabricates information to make up for memory loss)
Treatment is with thiamine but under 20% of patients respond.
On to 31.3... MS...
It is a chronic disorder, usually following Wernicke's encephalopathy.
The patient has an inability to consolidate new info, retrograde amnesia, patchy preservation of long term memory, a lack of insight and confabulates (=fabricates information to make up for memory loss)
Treatment is with thiamine but under 20% of patients respond.
On to 31.3... MS...
MRCP revision battle 31.3: Multiple Sclerosis
Multiple sclerosis is a cell-mediated autoimmune disorder characterised by plaques of demyelination at sites throughout the CNS but not in the peripheral nerves.
4 main types:
Initial presentation tends to be a single symptom, such as:
Diagnosis is by (NB none is specific):
Good prognostic factors are:
Risk of MS is increased 20-40% in siblings and there is 25% concordance in monozygotic twins.
Treatment is:
Now for the less heavy-going Menieres disease...
4 main types:
- relapsing-remitting
- accounts for 80% of cases
- secondary progressive
- up to 50% of relapsing-remitting patients eventually develop this
- primary progressive
- 10-15% of cases
- older age of onset
- progressive-relapsing
Initial presentation tends to be a single symptom, such as:
- optic neuritis
- pain on eye movement and rapid deterioration in central vision, loss of colour vision
- treatment is methylpred
- single episode gives 40-60% chance of subsquent MS
- numbness or tingling in limbs
- leg weakness
- ataxia
Diagnosis is by (NB none is specific):
- lesions disseminated in time and location
- T2 weighted MRI showing demyelinating plaques
- delayed visual evoked response potentials
- oligoclonal bands in CSF but not serum
Good prognostic factors are:
- relapsing-remitting course
- female
- young onset
- sensory symptoms
Risk of MS is increased 20-40% in siblings and there is 25% concordance in monozygotic twins.
Treatment is:
- IV methylprednisolone
- shortens relapses
- no effect on incidence of attacks
- beta interferon
- decreases relapses by 30%
- given if
- relapsing-remitting course and 2 relapses in 2 yrs and can walk 100m unaided
- secondary progressive and 2 relapses in 2 yrs and 100m aided
- side effect: flu-like
- baclofen
- decreases spascity
Now for the less heavy-going Menieres disease...
MRCP revision battle 31.4: Meniere's Disease
Meniere's Disease is a disorder of the inner ear causing vertigo and hearing loss.
Features include:
There may be nystagmus and a positive romberg's test
It is usually unilateral and is believed to be associated with endolymphatic hydrops (=increased fluid in ear)
Rarely it may be associated with drop attacks - no LOC or vertigo, but suddenly falling to one side.
Management:
Next up: that formally very topical topic CJD...
Features include:
- vertigo
- tinnitus
- sesorineural hearing loss
- aural fullness
There may be nystagmus and a positive romberg's test
It is usually unilateral and is believed to be associated with endolymphatic hydrops (=increased fluid in ear)
Rarely it may be associated with drop attacks - no LOC or vertigo, but suddenly falling to one side.
Management:
- prochlorperazine
- inform DVLA and stop driving until controlled.
Next up: that formally very topical topic CJD...
MRCP revision battle 31.5: CJD
Creutzfeldt-Jakob Disease (=CJD) is a prion disease which causes a rapidly progressive dementia with myoclonus.
The majority of cases are sporadic. There is also an inherited form and an acquired form (=varient CJD, from meat infected with BSE)
CSF examination is usually normal but EEG shows characteristic biphasic high-amplitude sharp waves.
Death is usually within 6 months.
On a lighter note lets look at herpes zoster opthalmicus...
The majority of cases are sporadic. There is also an inherited form and an acquired form (=varient CJD, from meat infected with BSE)
CSF examination is usually normal but EEG shows characteristic biphasic high-amplitude sharp waves.
Death is usually within 6 months.
On a lighter note lets look at herpes zoster opthalmicus...
MRCP revision battle 31.6: Herpes Zoster Opthalmicus
Herpes zoster opthalmicus is the reactivation of varicella zoster in the area supplied by the opthalmic division of the trigeminal nerve.
It occurs in roughly 10% of cases of shingles.
There may be Hutchinson's sign = rash on the tip of nose, which indicates nasocillary involvement and is a strong risk factor for ocular involvement.
Treatment is oral antivirals for 7 to 10 days and urgent opthalmic review if there is ocular involvement.
On to the final revision battle of the day...
It occurs in roughly 10% of cases of shingles.
There may be Hutchinson's sign = rash on the tip of nose, which indicates nasocillary involvement and is a strong risk factor for ocular involvement.
Treatment is oral antivirals for 7 to 10 days and urgent opthalmic review if there is ocular involvement.
On to the final revision battle of the day...
MRCP revision battle 31.7: Ramsey Hunt Syndrome
Ramsey Hunt Syndrome is the reactivation of varicella zoster in the geniculate ganglion of the facial nerve.
It is characterised by:
Treatment is with oral antivirals
It is characterised by:
- herpes zoster oticus (=herpetic eruption in external auditory meatus)
- facial nerve palsy
- +/- deafness, tinnitus and vertigo
Treatment is with oral antivirals
Friday, 15 October 2010
MRCP revision battle 30.1: Retinitis Pigmentosa
Today is the start of a 3 day neuro/opthalmology blitz, so hold on to your hats....
MRCP revision battle 30.1: Retinitis Pigmentosa
MRCP revision battle 30.2: Oculogyric Crisis
MRCP revision battle 30.3: Myotonic Dystrophy
MRCP revision battle 30.4: Trinucleotide repeat disorders
MRCP revision battle 30.5: Huntington's Chorea
MRCP revision battle 30.6: Friedreich's ataxia
MRCP revision battle 30.7: Alzheimer's Disease
MRCP revision battle 30.1: Retinitis Pigmentosa
Retinitis pigmentosa is a type of progressive retinal dystrophy which eventually leads to blindness.
It has a very characteristic fundoscopic appearence with black mottling of the retina and a pale optic disc, as illustrated below in an image by Christian Hammel (from wiki commons):

It can be inherited in an autosomal dominant, autosomal recessive or X linked recessive fashion.
Night blindness is often the first sign.
Later comes funnel/tunnel vision.
It is associated with many conditions, including:
There is no cure for retinitis pigmentosa but progression of the disease can be slowed by vitamin A.
On to the second battle of the day...
MRCP revision battle 30.1: Retinitis Pigmentosa
MRCP revision battle 30.2: Oculogyric Crisis
MRCP revision battle 30.3: Myotonic Dystrophy
MRCP revision battle 30.4: Trinucleotide repeat disorders
MRCP revision battle 30.5: Huntington's Chorea
MRCP revision battle 30.6: Friedreich's ataxia
MRCP revision battle 30.7: Alzheimer's Disease
MRCP revision battle 30.1: Retinitis Pigmentosa
Retinitis pigmentosa is a type of progressive retinal dystrophy which eventually leads to blindness.
It has a very characteristic fundoscopic appearence with black mottling of the retina and a pale optic disc, as illustrated below in an image by Christian Hammel (from wiki commons):
It can be inherited in an autosomal dominant, autosomal recessive or X linked recessive fashion.
Night blindness is often the first sign.
Later comes funnel/tunnel vision.
It is associated with many conditions, including:
- Kearns Sayre (remember battle 15.1?)
- Ushers syndrome = retinitis pigmentosa with sensorineural deafness
- congenital toxoplasmosis
There is no cure for retinitis pigmentosa but progression of the disease can be slowed by vitamin A.
On to the second battle of the day...
MRCP revision battle 30.2: Oculogyric Crisis
The key features of an oculogyric crisis are restlessness and upward deviation of the eyes (although this only occurs in severe cases).
Oculogyric crises may be precipitated by a range of drugs including:
Several clinical conditions can also cause oculogyric crises, for example:
Treatment is with procyclidine, an anticholinergic.
On to the next battle...
Oculogyric crises may be precipitated by a range of drugs including:
- neuroleptics
- metoclopramide/domperidone
- nifedipine
- TCA
- carbamazepine
Several clinical conditions can also cause oculogyric crises, for example:
- parkinsons disease
- post encephalitis
- bilateral thalmic infarction
- MS
Treatment is with procyclidine, an anticholinergic.
On to the next battle...
MRCP revision battle 30.3: Myotonic Dystrophy
Myotonic dystrophy is an autosomal dominant condition in which there is muscle weakness and myotonia. It is a trinucleotide repeat disorder.
Onset tends to be in the 30s.
There are 2 types:
Dystrophia myotonica (=DM) 1
Features associated with myotonic dystrophy include:
It is incurable but phenytoin can improve the myotonia.
Lets move on to consider an overview of trinucleotide repeat disorders
Onset tends to be in the 30s.
There are 2 types:
Dystrophia myotonica (=DM) 1
- 98% of cases
- more severe
- distal muscle weakness
- chromosome 19
- 2% of cases
- less severe
- proximal muscle weakness
- chromosome 3
Features associated with myotonic dystrophy include:
- long faces
- frontal baldness
- myotonia and weakness
- testicular/ovarian atrophy
- bilateral ptosis
- cateract
- cardiomyopathy
- diabetes
- miotic pupils
- mildly decreased IQ
It is incurable but phenytoin can improve the myotonia.
Lets move on to consider an overview of trinucleotide repeat disorders
MRCP revision battle 30.4: Trinucleotide repeat disorders
Trinucleotide repeat disorders are conditions in which 3 nucleotides in the DNA are expanded.
The most 'famous' are:
Two concepts to be born in mind for trinucleotide repeat disorders are:
Anticipation = the disease presents earlier and is worse in successive generations
Somatic instability = expansion increases as patient gets older
So lets briefly cover the most famous, Huntingtons...
The most 'famous' are:
- Huntingtons chorea (CAG) - covered in next battle
- Fragile X (CGG)
- Myotonic dystrophy (CTG) - covered in previous battle
- Friedreichs ataxia (GAA) - covered in battle 30.6
Two concepts to be born in mind for trinucleotide repeat disorders are:
Anticipation = the disease presents earlier and is worse in successive generations
Somatic instability = expansion increases as patient gets older
So lets briefly cover the most famous, Huntingtons...
MRCP revision battle 30.5: Huntington's Chorea
Huntington's chorea is an autosomal dominant condition due to CAG repeats.
It is carried on chromosome 4.
Symptoms tend to start in the 40s with a progression from chorea to irritability to dementia and death.
There is no cure. The chorea may be treated with a dopamine antagonist such as tetrabenazine.
Note that Hunington's has complete penetrance so a child of a sufferer has a 50% chance of being affected. Due to anticipation if they are affected they are also likely to develop symptoms earlier.
Next up: Friedreich's ataxia...
It is carried on chromosome 4.
Symptoms tend to start in the 40s with a progression from chorea to irritability to dementia and death.
There is no cure. The chorea may be treated with a dopamine antagonist such as tetrabenazine.
Note that Hunington's has complete penetrance so a child of a sufferer has a 50% chance of being affected. Due to anticipation if they are affected they are also likely to develop symptoms earlier.
Next up: Friedreich's ataxia...
MRCP revision battle 30.6: Friedreich's ataxia
Friedreichs ataxia is an autosomal recessive trinucleotide repeat disorder (GAA)
It causes degeneration of nerve tracts resulting in cerebellar ataxia, dysarthria, nystagmus and dysdiadocholokinesis.
Muscles are weak, reflexes are depressed but plantars are upgoing.
There is often scoliosis and high arches of the feet.
Cardiomyopathy is another complication.
There is no cure.
Lets now try and forget all these incurable diseases with a touch of Alzheimer's...
It causes degeneration of nerve tracts resulting in cerebellar ataxia, dysarthria, nystagmus and dysdiadocholokinesis.
Muscles are weak, reflexes are depressed but plantars are upgoing.
There is often scoliosis and high arches of the feet.
Cardiomyopathy is another complication.
There is no cure.
Lets now try and forget all these incurable diseases with a touch of Alzheimer's...
MRCP revision battle 30.7: Alzheimer's Disease
Alzheimer's disease is the leading cause of dementia. This battle aims to pick out a few juicy facts for MRCP; http://alzheimers.org.uk/ can provide more in-depth information if you are interested.
The earliest symptom of AD is typically forgetfulness.
5% of cases are autosomal dominant, with chromosomes 1, 14, 19 and 21 implimented.
After age, apoE4 (chromosome 19) is the most significant risk factor for AD.
Beta amyloid plaques and hyperphosphorylated tau protein tangles are found within neurones post-mortem.
The density of the tangles can correlate with the severity of the dementia.
Hippocampal atrophy is prominant.
Cholinesterase inhibitors such as donepezil, rivastigmine and galantamine are licensed for patients with a MMSE of between 10 and 20.
Memantine (an antiglutamatergic) may be useful in severe AD.
As Bugs Bunny would say, thhhhatttttts alll folllkkkksss.... until tomorrow!
The earliest symptom of AD is typically forgetfulness.
5% of cases are autosomal dominant, with chromosomes 1, 14, 19 and 21 implimented.
After age, apoE4 (chromosome 19) is the most significant risk factor for AD.
Beta amyloid plaques and hyperphosphorylated tau protein tangles are found within neurones post-mortem.
The density of the tangles can correlate with the severity of the dementia.
Hippocampal atrophy is prominant.
Cholinesterase inhibitors such as donepezil, rivastigmine and galantamine are licensed for patients with a MMSE of between 10 and 20.
Memantine (an antiglutamatergic) may be useful in severe AD.
As Bugs Bunny would say, thhhhatttttts alll folllkkkksss.... until tomorrow!
Thursday, 14 October 2010
MRCP revision battle 29.1: Hypoglycaemia
After nearly a week away I'm back with a bumper set of battles, the first of which is hypoglycaemia, which has been a recurring theme in both my patients and myself this week! Enjoy!
MRCP revision battle 29.1: Hypoglycaemia
MRCP revision battle 29.2: Thyroid eye disease
MRCP revision battle 29.3: Hyperlipidaemia
MRCP revision battle 29.4: Lipid-lowering treatment
MRCP revision battle 29.5: Restless legs syndrome
MRCP revision battle 29.6: Histocytosis X
MRCP revision battle 29.7: Bartter's Syndrome
MRCP revision battle 29.8: Gitelman Syndrome
MRCP revision battle 29.9: Liddle's Syndrome
MRCP revision battle 29.1: Hypoglycaemia
Hypoglycaemia is defined as plasma glucose <3mmol/l.
In general in diabetics autonomic symptoms of hypoglycaemia (sweating, anxiety, tremor, palpitations) occur below 3.5mmol and neurological symptoms (confusion, drowsiness, seizures, coma) occur below 2.5mmol.
If a diabetic has frequent hypos they may become 'insensitive' and no longer experience symptoms before becoming unresponsive. Symptoms may be 'restored' by carefully avoiding hypos for 3 months.
Causes of hypoglycaemia are easy to remember as it "IS PLAIN" to see...
Take bloods for glucose, insulin, c-peptide and plasma ketones.
Normal/high insulin, no ketones: insulinoma, drugs
Insulin low, no ketones: non-pancreatic neoplasm
Insulin low, ketones high: alcohol, addissons, pituitary insufficiency.
Post-pradial hypoglycaemia can occur post-gastrectomy
Whipples Triad is a set of criteria which if fulfilled suggest a patient's symptoms are due to hypoglycaemia:
Treatment
I'm sure this is all old-hat to you all... get the pt to eat if they can, 1mg IM glucagon if they can't and no IV access (remember glucagon effects only last for 20 mins and may not work at all in alcoholics) and if IV is an option the 50mls of 50% glucose or the more modern 200mls of 10% (less abrasive to the veins)
Now for some TED time...
MRCP revision battle 29.1: Hypoglycaemia
MRCP revision battle 29.2: Thyroid eye disease
MRCP revision battle 29.3: Hyperlipidaemia
MRCP revision battle 29.4: Lipid-lowering treatment
MRCP revision battle 29.5: Restless legs syndrome
MRCP revision battle 29.6: Histocytosis X
MRCP revision battle 29.7: Bartter's Syndrome
MRCP revision battle 29.8: Gitelman Syndrome
MRCP revision battle 29.9: Liddle's Syndrome
MRCP revision battle 29.1: Hypoglycaemia
Hypoglycaemia is defined as plasma glucose <3mmol/l.
In general in diabetics autonomic symptoms of hypoglycaemia (sweating, anxiety, tremor, palpitations) occur below 3.5mmol and neurological symptoms (confusion, drowsiness, seizures, coma) occur below 2.5mmol.
If a diabetic has frequent hypos they may become 'insensitive' and no longer experience symptoms before becoming unresponsive. Symptoms may be 'restored' by carefully avoiding hypos for 3 months.
Causes of hypoglycaemia are easy to remember as it "IS PLAIN" to see...
- Insulin
- Sulphonyureas/other drugs
- Pituitary insufficiency
- Liver failure
- Addisons disease or alcohol
- Insulinoma
- Neoplasms eg retroperitoneal fibrosarcomas than secrete IGF
Take bloods for glucose, insulin, c-peptide and plasma ketones.
Normal/high insulin, no ketones: insulinoma, drugs
Insulin low, no ketones: non-pancreatic neoplasm
Insulin low, ketones high: alcohol, addissons, pituitary insufficiency.
Post-pradial hypoglycaemia can occur post-gastrectomy
Whipples Triad is a set of criteria which if fulfilled suggest a patient's symptoms are due to hypoglycaemia:
- symptoms suggestive of hypoglycaemia
- BM < or equal to 2.5
- symptoms relieved by food.
Treatment
I'm sure this is all old-hat to you all... get the pt to eat if they can, 1mg IM glucagon if they can't and no IV access (remember glucagon effects only last for 20 mins and may not work at all in alcoholics) and if IV is an option the 50mls of 50% glucose or the more modern 200mls of 10% (less abrasive to the veins)
Now for some TED time...
MRCP revision battle 29.2: Thyroid eye disease
Thyroid eye disease, referred to by its friends as 'TED', can occur in people who are hyperthyroid, hypothyroid or euthyroid.
Thyrotoxicosis from any cause can cause lid lag and lid retraction.
However, only Graves disease causes:
(as an aside, I've always been mystified by the difference between proptosis and exophthalmos. Unfortunately it appears I'm not the only one as some sources suggest the difference is related to the degree of protrusion whilst others say exophthalmos is used if the aetiology is endocrine and proptosis is used if the aetiology is not endocrine...)
25-50% of patients with Grave's disease have TED.
Risk of TED is increased in smokers.
The danger of TED is optic nerve compression. Symptoms/signs of optic nerve compression include:
Treatment for TED is topical lubricants, steroids if severe and possibly even surgery.
Now for a horrid battle with hyperlipidaemia...
Thyrotoxicosis from any cause can cause lid lag and lid retraction.
However, only Graves disease causes:
- periorbital oedema
- conjunctivial injection
- proptosis/exophthalmos
- opthalmoplegia/diplopia
- papilloedema
(as an aside, I've always been mystified by the difference between proptosis and exophthalmos. Unfortunately it appears I'm not the only one as some sources suggest the difference is related to the degree of protrusion whilst others say exophthalmos is used if the aetiology is endocrine and proptosis is used if the aetiology is not endocrine...)
25-50% of patients with Grave's disease have TED.
Risk of TED is increased in smokers.
The danger of TED is optic nerve compression. Symptoms/signs of optic nerve compression include:
- blurred vision/decrease VA
- decreased colour vision
- a relative afferent papillary defect
Treatment for TED is topical lubricants, steroids if severe and possibly even surgery.
Now for a horrid battle with hyperlipidaemia...
MRCP revision battle 29.3: Hyperlipidaemia
This battle is quickly going to get complex and aims only to be an MRCP-focused overview rather than a comprehensive discussion. It is divided into 5 stages:
1. The Basics
Hyperlipidaemia = raised lipids. Lipids come in 4 main 'flavours':
Signs:
So lets look first at cholesterol and hypercholesterolaemia.
2. Hypercholesterolamia
a. Familial
b. Acquired
3. HDL
HDL is 'good' cholesterol
It is higher in:
It is lower in:
4. Hypertriglyceridaemia
a. Familial
b. Secondary
5. Mixed hyperlipidaemia
After that wordy and depressing battle, lets move on to treatment of hyperlipidaemia...
- The basics
- Hypercholesterolaemia
- HDL - the good cholesterol
- Hypertriglyceridaemia
- Mixed
1. The Basics
Hyperlipidaemia = raised lipids. Lipids come in 4 main 'flavours':
- chylomicrons = carry triglyceride
- LDL = mainly cholesterol (50%, 10% TG) = the 'bad' flavour
- HDL = mainly phospholipid = the 'good' flavour, carry cholesterol back to the liver
- VLDL = mainly triglyceride (60%, 20% cholesterol)
Signs:
- corneal arcus = grey-white ring around cornea
- xanthelasma = yellow collection of cholesterol under skin
- xanthomata = 'lumps' of cholesterol
- eruptive xanthomata = small yellow-orange papules that appear all over body
- lipaemia retinalis = 'creamy' appearence of blood vessels on fundoscopy
So lets look first at cholesterol and hypercholesterolaemia.
2. Hypercholesterolamia
a. Familial
- LDL receptor dysfunction
- cholesterol 7.5-16
- raised LDL
- tendon xanthomata, corneal arcus and xanthelasma
- heterozygous prevalance 1/500 --> MI in 40s
- homozygous --> MI in 20s
- Polygenic hypercholesterolaemia
- cholesterol 6.5-9
- raised LDL
- xanthelasma and corneal arcus
b. Acquired
- nephrotic syndrome
- renal transplant
- cholestasis
- hypothyroidism
3. HDL
HDL is 'good' cholesterol
It is higher in:
- thin people
- exercise
- oestrogens
- alcohol
- low triglycerides
It is lower in:
- obesity
- sedentary states
- post-puberty males
- smoking
4. Hypertriglyceridaemia
a. Familial
- failure to metabolise chylomicrcons
- features include:
- eruptive xanthomata
- lipaemia retinalis
- retinal vein thrombosis
- pancreatitis
- hepatosplenomegaly
b. Secondary
- diabetes
- obestiy
- alcohol
- chronic renal failure
- liver disease
- drugs such as thiazides, beta blockers or oestrogens
5. Mixed hyperlipidaemia
- Look for palar xanthomas and tuberous xanthomas
After that wordy and depressing battle, lets move on to treatment of hyperlipidaemia...
MRCP revision battle 29.4: Lipid-lowering treatment
NICE recommends that all those with a 10 yr cardiovascular risk of >20% should be offered lipid-lowering therapy.
1st line: 40mg simvastatin
Measure LFTs when starting, at 3 months and at 12 months.
In primary prevention there is no 'target' cholesterol
In secondary prevention the target is less than 4mmol/l cholesterol and less than 2mmol/l LDL
If statins are not tolerated consider:
Mechanisms of action
Statins are HMG CoA reductase inhibitors. They therefore work by decreasing the production of cholesterol in the liver. The decreased production of cholesterol in the liver also results in the liver absorbing and processing more LDL, hence further reducing cholesterol.
Grapefruit juice decreases the metabolism of statins. Patients on statins are therefore advised to avoid grapefruit juice as it would increase the risk of the rare side effect of rhabdomyolysis
Ezetimibe works by preventing intestinal absorption of cholesterol.
Fibrates are PPAR alpha receptor agonists. They therefore increase clearance of VLDL and remnant particles and decrease TG secreation.
Fibrates and statins tend not to be used together due to increased risk of rhabdomyolysis.
Nicotinic acid (=vitamin B3) blocks breakdown of fats in adipose tissue.
It can cause facial flushing.
1st line: 40mg simvastatin
Measure LFTs when starting, at 3 months and at 12 months.
In primary prevention there is no 'target' cholesterol
In secondary prevention the target is less than 4mmol/l cholesterol and less than 2mmol/l LDL
If statins are not tolerated consider:
- fibrates
- ezetimibe
- nicotinic acid
Mechanisms of action
Statins are HMG CoA reductase inhibitors. They therefore work by decreasing the production of cholesterol in the liver. The decreased production of cholesterol in the liver also results in the liver absorbing and processing more LDL, hence further reducing cholesterol.
Grapefruit juice decreases the metabolism of statins. Patients on statins are therefore advised to avoid grapefruit juice as it would increase the risk of the rare side effect of rhabdomyolysis
Ezetimibe works by preventing intestinal absorption of cholesterol.
Fibrates are PPAR alpha receptor agonists. They therefore increase clearance of VLDL and remnant particles and decrease TG secreation.
Fibrates and statins tend not to be used together due to increased risk of rhabdomyolysis.
Nicotinic acid (=vitamin B3) blocks breakdown of fats in adipose tissue.
It can cause facial flushing.
For the really keen:
NICE lipid modification guide
After those heavy-going battles lets tackle something light - restless legs syndrome...
MRCP revision battle 29.5: Restless legs syndrome
Restless legs syndrome, sometimes known as Ekbom's syndrome, is a condition in which a person has unpleasant sensations in their legs and a desire to move them.
Restless legs may be idiopathic or secondary to:
1st line treatments are dopamine agonists such as pramipexole
2nd line treatments include benzodiazepines or gabapentin.
To keep the neurones jumping lets move on to a completely different topic again - histiocytosis X...
Restless legs may be idiopathic or secondary to:
- pregnancy
- iron deficiency
- ureamia
- diabetes
- RA
1st line treatments are dopamine agonists such as pramipexole
2nd line treatments include benzodiazepines or gabapentin.
To keep the neurones jumping lets move on to a completely different topic again - histiocytosis X...
MRCP revision battle 29.6: Histiocytosis X
Histocytosis X, aka Langerhans-cell histiocytosis, is a group of disorders in which there is organ infiltration by granulomatous lesions containing clonally proliferated dendrintic (=Langerhams) cells.
The most commonly affected organs are lungs and bones.
Lung histiocytosis tends to affect young adults and is commonest in smokers.
The CXR shows multiple ring shadows with diffuse reticulo-nodular opacities affecting mainly the upper and mid zones.
Biopsy would show characteristic Birbeck granules.
Treatment is ?local excision, ?steroids.
Now onwards for a run of the last 3 short battles of the day, starting with Bartter's Syndrome...
The most commonly affected organs are lungs and bones.
Lung histiocytosis tends to affect young adults and is commonest in smokers.
The CXR shows multiple ring shadows with diffuse reticulo-nodular opacities affecting mainly the upper and mid zones.
Biopsy would show characteristic Birbeck granules.
Treatment is ?local excision, ?steroids.
Now onwards for a run of the last 3 short battles of the day, starting with Bartter's Syndrome...
MRCP revision battle 29.7: Bartter's Syndrome
Bartter's Syndrome is an autosomal recessive condition in which there is defective chloride reabsorption in the Na-K-2Cl channels in the loop of Henle resulting in severe hypokalaemia.
It presents in childhood with failure to thrive and polyuria/polydipsia
Blood pressure is normal/low.
There is hyperreninaemia and hypertrophy of the JGA.
Treatment is with potassium replacement and NSAIDs.
Next... Gitelman Syndrome....
It presents in childhood with failure to thrive and polyuria/polydipsia
Blood pressure is normal/low.
There is hyperreninaemia and hypertrophy of the JGA.
Treatment is with potassium replacement and NSAIDs.
Next... Gitelman Syndrome....
MRCP revision battle 29.8: Gitelman Syndrome
Gitelman Syndrome is an autosomal recessive disorder in which there is decreased salt reabsorption in the distal tubule resulting in hypokalaemia due to secondary hyperaldosteronism.
Patients with Gitelman Syndrome have:
Treatment is magnesium and potassium replacement.
Finally - Liddles!
Patients with Gitelman Syndrome have:
- metabolic alkalosis
- low potassium
- low magnesium
- usually normal blood pressure
Treatment is magnesium and potassium replacement.
Finally - Liddles!
MRCP revision battle 29.9: Liddle's Syndrome
Liddle's syndrome is an autosomal dominant condition caused by enhanced sodium reabsorption in the DCT.
It results in:
Treatment is salt restriction, potassium, amiloride.
It results in:
- hypertension
- hypokalaemia
- metabolic alkalosis
Treatment is salt restriction, potassium, amiloride.
Saturday, 9 October 2010
MRCP revision battle 28.1: Haemochromatosis
I feel like I'm possibly starting to make some inroads into this MRCP revision thing, and my chocolate dependency level has decreased a little. Today is another random assortment of gems:
MRCP revision battle 28.1: Haemochromatosis
MRCP revision battle 28.2: Syphilis
MRCP revision battle 28.3: Third nerve palsy
MRCP revision battle 28.4: G6PD deficiency
MRCP revision battle 28.5: Kaposi's sarcoma
MRCP revision battle 28.6: Chronic Myeloid Leukaemia
MRCP revision battle 28.7: Gerstmann's Syndrome
MRCP revision battle 28.1: Haemochromatosis
Haemochromatosis is an excessive accumulation of iron.
There is increased intestinal absorption leading to deposition in joints, skin, the heart, liver, pancreas, adrenals and pituitary.
It is an autosomal recessive disorder, inherited on chromosome 6.
Presentation is initially with tiredness and arthralgia
Later problems include:
Males are affected earlier and more severely than females.
Diagnosis is by:
Treatment is regular venesection and ?chelation with desferrioxamine
Haemosiderosis is secondary haemochromatosis.
Causes of haemosiderosis include:
Thats enough iron for one day... onwards to some syphilis...
MRCP revision battle 28.1: Haemochromatosis
MRCP revision battle 28.2: Syphilis
MRCP revision battle 28.3: Third nerve palsy
MRCP revision battle 28.4: G6PD deficiency
MRCP revision battle 28.5: Kaposi's sarcoma
MRCP revision battle 28.6: Chronic Myeloid Leukaemia
MRCP revision battle 28.7: Gerstmann's Syndrome
MRCP revision battle 28.1: Haemochromatosis
Haemochromatosis is an excessive accumulation of iron.
There is increased intestinal absorption leading to deposition in joints, skin, the heart, liver, pancreas, adrenals and pituitary.
It is an autosomal recessive disorder, inherited on chromosome 6.
Presentation is initially with tiredness and arthralgia
Later problems include:
- diabetes mellitus (bronze diabetes)
- slate-grey skin
- liver disease/cirrhosis
- cardiac failure/cardiomegaly
- pseudogout
- hypopituitism
- >30% develop hepatocellular carcinoma
Males are affected earlier and more severely than females.
Diagnosis is by:
- transferrin saturation >50%
- ferritin >300-500micrograms/l (depending on guidelines)
- liver biopsy - Perls stain to show hepatic iron >180micromol/g
Treatment is regular venesection and ?chelation with desferrioxamine
Haemosiderosis is secondary haemochromatosis.
Causes of haemosiderosis include:
- beta thalassemia
- sideroblastic anaemia
- aplastic anaemia
- transfusions
- alcoholic cirrhosis
- chronic viral hepatitis
- porphyria cutanea tarda
Thats enough iron for one day... onwards to some syphilis...
MRCP revision battle 28.2: Syphillis
Syphilis is another of those conditions which is a common differential in MRCP questions.
Syphilis is caused by the spirochaete treponema pallidum.
There are 4 stages of syphilis:
1) Primary
2) Secondary
3) Tertiary syphilis
4) Quaternary syphilis
Tests:
Treatment:
Random eponymous warning - Jarisch-Herxheimer reaction:
Now on for a bit of third nerve palsy....
Syphilis is caused by the spirochaete treponema pallidum.
There are 4 stages of syphilis:
1) Primary
- painless genital ulcer
- known as a chancre
- highly infectious
2) Secondary
- occurs 4-8 weeks after the chancre
- rash, malaise, lymphadenopathy, temperature
- condylomata lata
3) Tertiary syphilis
- >2yrs after secondary
- gummas (=granulomas) form in skin, mucosa and viscera
4) Quaternary syphilis
- cardiovascular
- aortic aneurysm
- aortic regurgitation
- neurosyphilis
- cranial nerve palsies
- general paralysis of the insane
- tabes dorsalis
- sensory ataxia
- numb legs
- lightening pains
- upgoing plantars
- argyll robertson pupil
Tests:
- cardiolipin antibody = VDRL, RPR
- not syphilis specific
- insensitive in late syphillis
- becomes negative after treatment
- false +ives in pregnancy, SLE, TB, leprosy, malaria, HIV
- treponeme-specific antibody = TPHA
- remains positive after treatment
- dark ground microscopy
Treatment:
- IM penicillin or PO doxcycline
Random eponymous warning - Jarisch-Herxheimer reaction:
- raised pulse, temp and vasodilation
- occurs hours after 1st dose of antibiotics
- due to release of endotoxin
Now on for a bit of third nerve palsy....
MRCP revision battle 28.3: Third nerve palsy
Cranial nerve III = oculomotor nerve arises in the rostral midbrain at the level of the superior colliculus.
It has 2 adjacent nuclei:
The oculomotor nerve passes between the posterior cerebral and superior cerebellar arteries, then on through the cavernous sinus and out through the superior orbital fissure.
In the orbit it splits into:
Complete 3rd nerve palsies tend to be peripheral rather than central in origin as the nucleus is big.
Classic 3rd nerve palsy:
If the pupil is spared it is sometimes referred to as a 'medical' third nerve palsy, whereas if it is fixed and dilated it is a 'surgical' third nerve palsy.
The reasoning behind this is that the visceral constrictive fibres run on the outside of the nerve so are spared in vascular aetiologies.
Causes of third nerve palsy:
Webers syndrome: ipsilateral third nerve palsy with contralateral hemiplegia --> signifies a midbrain stroke.
After that pleasant forray into the world of neurology on to something completely different - G6PD deficiency...
It has 2 adjacent nuclei:
- oculomotor nucleus - somatic fibres (eye movements)
- edinger-westphal nucleus - visceral fibres (pupillary constriction)
The oculomotor nerve passes between the posterior cerebral and superior cerebellar arteries, then on through the cavernous sinus and out through the superior orbital fissure.
In the orbit it splits into:
- superior branch - supplies levator palpebrae
- inferior branch - supplies medial rectus, inferior rectus and inferior oblique muscles and carries the visceral fibres
Complete 3rd nerve palsies tend to be peripheral rather than central in origin as the nucleus is big.
Classic 3rd nerve palsy:
- ptosis
- 'down and out' pupil
- dilated pupil
If the pupil is spared it is sometimes referred to as a 'medical' third nerve palsy, whereas if it is fixed and dilated it is a 'surgical' third nerve palsy.
The reasoning behind this is that the visceral constrictive fibres run on the outside of the nerve so are spared in vascular aetiologies.
Causes of third nerve palsy:
- diabetes (75% pupil-sparing)
- temporal arteritis
- SLE
- MS
- cavernous sinus thrombosis
- amyloid
- posterior communicating artery aneurysm (usually painful)
- tumour
Webers syndrome: ipsilateral third nerve palsy with contralateral hemiplegia --> signifies a midbrain stroke.
After that pleasant forray into the world of neurology on to something completely different - G6PD deficiency...
MRCP revision battle 28.4: G6PD deficiency
Glucose-6-phosphate dehydrogenase deficiency is the commonest RBC enzyme defect.
It is x-linked recessive.
It causes intravascular haemolysis.
Generally patients are asymptomatic unless a crisis is precipitated, in which case they become anaemic and jaundiced.
Precipitants of crisis include:
During a crisis a blood film will show:
Management is to avoid precipitants and transfuse if necessary.
On to Kaposi's sarcoma...
It is x-linked recessive.
It causes intravascular haemolysis.
Generally patients are asymptomatic unless a crisis is precipitated, in which case they become anaemic and jaundiced.
Precipitants of crisis include:
- drugs
- primaquine
- sulfonamides
- ciprofloxacin
- aspirin
- broad/fava beans
- illness
During a crisis a blood film will show:
- bite cells
- heinz bodies (=inclusions within RBCs of denatured haemoglobin)
Management is to avoid precipitants and transfuse if necessary.
On to Kaposi's sarcoma...
MRCP revision battle 28.5: Kaposi's sarcoma
Kaposi's sarcoma is a red, brown, purple or blue plaque on the skin or mucosa

Kaposi's sarcoma is derived from capillary endothelial cells or fibrous tissue.
It is associated with HHV-8.
It may be secondary to immunosupression, or a diagnosing feature of HIV infection.
Next up - CML....
Kaposi's sarcoma is derived from capillary endothelial cells or fibrous tissue.
It is associated with HHV-8.
It may be secondary to immunosupression, or a diagnosing feature of HIV infection.
Next up - CML....
MRCP revision battle 28.6: Chronic Myeloid leukaemia
Chronic myeloid leukaemia is an uncontrolled clonal proliferation of myeloid cells.
It tends to affect middle aged people (40 to 60 years)
Classical presentation is with:
Possible additional presentations are:
Approximately 30% are detected by chance.
Features include:
The philadelphia chromosome is present in >80% of cases
The philadelphia chromosome:
Treatment for CML is:
CML transforms to AML in 80% of cases and ALL in 20%
Last battle of the day is Gertmann's Syndrome...
It tends to affect middle aged people (40 to 60 years)
Classical presentation is with:
- decreased weight
- tiredness
- sweating
Possible additional presentations are:
- gout due to increased purine breakdown
- abdo pain due to splenomegaly
- bleeding due to platelet dysfunction
Approximately 30% are detected by chance.
Features include:
- elevated WCC - often 100-500
- massive neutrophilia with left shift
- low neutrophil alkaline phosphatase
- splenomegaly in >75%
The philadelphia chromosome is present in >80% of cases
The philadelphia chromosome:
- is a hybrid chromosome formed by t(9;22)
- forms a gene BCR-ABL which results in excess tyrosine kinase activity
- found in 80% CML, 5% children with ALL, 25% of adult ALL and 1% adult AML.
- is associated with a good prognosis in CML but a poor prognosis in all other leukaemias
Treatment for CML is:
- hydroxyurea
- imatimib = glivec = specific BCR-ABL tyrosine kinase inhibitor
- bone marrow transplant
CML transforms to AML in 80% of cases and ALL in 20%
Last battle of the day is Gertmann's Syndrome...
MRCP revision battle 28.7: Gerstmann's Syndrome
Gerstmann's Syndrome is a condition characteristed by:
Gerstmann's Syndrome is associated with lesions in the dominant brain hemisphere in the region of the angular gyrus of the parietal lobe.
On that esoteric note, see you tomorrow!
- dysgraphia
- dyscalculia
- finger agnosia
- left-right disorientation
Gerstmann's Syndrome is associated with lesions in the dominant brain hemisphere in the region of the angular gyrus of the parietal lobe.
On that esoteric note, see you tomorrow!
Friday, 8 October 2010
MRCP revision battle 27.1: Heparin induced thrombocytopenia (HIT)
Today we have an epic set of battles with some real hard-hitters hidden amongst them, including sarcoidosis which is a differential for around 110% of MRCP questions (or at least thats what it feels like) But if you get to the last battle you will be rewarded with lots of pictures (the joys of poikilocytosis) and then a link to look at some interesting non-medical pictures...
So the carrot is dangled, and here are the sticks:
MRCP revision battle 27.1: Heparin induced thrombocytopenia (HIT)
MRCP revision battle 27.2: Sarcoidosis
MRCP revision battle 27.3: Lofgren's syndrome
MRCP revision battle 27.4: Pancreatitis
MRCP revision battle 27.5: Visual field defects
MRCP revision battle 27.6: Paroxysmal nocturnal haemoglobinuria
MRCP revision battle 27.7: Poikilocytosis
MRCP revision battle 27.1: Heparin induced thrombocytopenia (HIT)
Heparin induced thrombocytopenia is one of those fabulous conditions whose name explains it all: low platelets, caused by heparin. It is often abbreviated to HIT, which confused me greatly when I first had a patient affected by it and my consultant declared "ah, he's got HIT" which made me wonder who he was suspecting of abuse on the ward...
Technically there are 2 types of HIT:
However, when HIT is mentioned, people generally mean type 2.
HIT is caused by antibodies against the heparin-platelet factor 4 complex. These antibodies can be found in 90% of patients with HIT... but may also be present in unaffected patients taking heparin.
Ironically, although HIT is characterised by low platelets it is an incredibly pro-thrombotic condition. As a result patients are likely to get PEs/DVTs and warfarin must absolutely not be started (since warfarin is initially prothrombotic too). As you can see HIT causes something of a management problem - thrombosis due to the treatment you would give for thrombosis...
Management of HIT will involve specialist haematological input but in terms of MRCP question answers think:
Note that HIT is more likely with unfractionated than LMW heparin.
Onwards to sarcoidosis...
So the carrot is dangled, and here are the sticks:
MRCP revision battle 27.1: Heparin induced thrombocytopenia (HIT)
MRCP revision battle 27.2: Sarcoidosis
MRCP revision battle 27.3: Lofgren's syndrome
MRCP revision battle 27.4: Pancreatitis
MRCP revision battle 27.5: Visual field defects
MRCP revision battle 27.6: Paroxysmal nocturnal haemoglobinuria
MRCP revision battle 27.7: Poikilocytosis
MRCP revision battle 27.1: Heparin induced thrombocytopenia (HIT)
Heparin induced thrombocytopenia is one of those fabulous conditions whose name explains it all: low platelets, caused by heparin. It is often abbreviated to HIT, which confused me greatly when I first had a patient affected by it and my consultant declared "ah, he's got HIT" which made me wonder who he was suspecting of abuse on the ward...
Technically there are 2 types of HIT:
- Type 1 - occurs in first 2 days, is non-immune and the platelet count spontaneously recovers
- Type 2 - occurs 4 to 10 days after starting heparin, is immune-mediated and potentially life-threatening.
However, when HIT is mentioned, people generally mean type 2.
HIT is caused by antibodies against the heparin-platelet factor 4 complex. These antibodies can be found in 90% of patients with HIT... but may also be present in unaffected patients taking heparin.
Ironically, although HIT is characterised by low platelets it is an incredibly pro-thrombotic condition. As a result patients are likely to get PEs/DVTs and warfarin must absolutely not be started (since warfarin is initially prothrombotic too). As you can see HIT causes something of a management problem - thrombosis due to the treatment you would give for thrombosis...
Management of HIT will involve specialist haematological input but in terms of MRCP question answers think:
- stop heparin
- stop/reverse warfarin
- give lepirudin (=highly specific direct inhibitor of thrombin)
Note that HIT is more likely with unfractionated than LMW heparin.
Onwards to sarcoidosis...
MRCP revision battle 27.2: Sarcoidosis
Sarcoidosis is a multi-system granulomatous disorder of unknown cause.
It is asymptomatic in up to 40% of cases, being discovered incidentally on a routine CXR.
Features of sarcoidosis may be divided into pulmonary and non-pulmonary:
Pulmonary features of sarcoidosis:
Non-pulmonary features of sarcoidosis include:
90% of patients with sarcoid will have an abnormal CXR.
Staging of CXR in sarcoid is:
Investigations:
Management:
Lets move on to briefly consider lofgrens syndrome...
It is asymptomatic in up to 40% of cases, being discovered incidentally on a routine CXR.
Features of sarcoidosis may be divided into pulmonary and non-pulmonary:
Pulmonary features of sarcoidosis:
- dry cough
- progressive dyspnoea
- chest pain
Non-pulmonary features of sarcoidosis include:
- lymphadenopathy (commonest in non-whites)
- erythema nodosum (commonest in white females)
- polyarthralgia
- hepatomegaly
- splenomegaly (around 25%)
- anterior uveitis (around 25%)
- glaucoma
- Bells palsy
- lupus pernio
- hypercalcaemia
- renal stones
- pituitary dysfunction
- cardiomyopathy...
90% of patients with sarcoid will have an abnormal CXR.
Staging of CXR in sarcoid is:
- 0 = clear CXR
- 1 = bilateral hilar lymphadenopathy
- 2 = bilateral hilar lymphadenopathy plus pulmonary infiltration
- 3 = pulmonary infiltration only
- 4 = fibrosis, honeycombing, pleural involvement
Investigations:
- raised ESR
- lymphopenia
- raised LFTs
- raised serum ACE
- raised calcium (5%)
- tuberculin skin test is positive in around a third
Management:
- BHL alone doesn't need treatment
- acute sarcoidosis : NSAIDs and bed rest
- prednisolone ( 40mg OD for 4-6 weeks then reducing dose over one year) is indicated if:
- parachymal lung disease
- uveitis
- hypercalcaemia
- neurological/cardiac involvement
Lets move on to briefly consider lofgrens syndrome...
MRCP revision battle 27.3: Lofgren's syndrome
Lofgrens syndrome is a subtype of sarcoidosis, characterised by:
It affects females more than males (85:15)
It carries a good prognosis - unlike sarcoidosis is unlikely to become chronic and most cases resolve in 6 months to 2 years.
On to something which often doesn't have a good prognosis... pancreatitis...
- erythema nodosum
- bilateral hilar lymphadenopathy
- fever
- athralgia
It affects females more than males (85:15)
It carries a good prognosis - unlike sarcoidosis is unlikely to become chronic and most cases resolve in 6 months to 2 years.
On to something which often doesn't have a good prognosis... pancreatitis...
MRCP revision battle 27.4: Pancreatitis
Acute pancreatitis tends to present as epigastric/central abdominal pain radiating to the back with vomiting. The pain may be improved by sitting forward.
Signs may be few; periumbilical discoloration (Cullen's sign) or flank discoloration (Grey Turner's sign) are rare.
Causes of pancreatitis can be remembered by I GET SMASHED:
Investigations:
Modified Glasgow criteria (helpfully spells out 'pancreas'):
Management of acute pancreatitis is:
Complications of pancreatitis include:
Now for something completely different, visual field defects...
Signs may be few; periumbilical discoloration (Cullen's sign) or flank discoloration (Grey Turner's sign) are rare.
Causes of pancreatitis can be remembered by I GET SMASHED:
- idiopathic
- gallstones
- ethanol
- trauma
- steroids
- mump
- autoimmune
- scorpion venom
- hyperlipidaemia, hypercalcaemia, hypothermia
- ERCP
- drugs (steroids, ocreotide, sulphonamides, tetracyclines, azathioprine, sodium valproate)
Investigations:
- bloods including amylase
- note amylase normalises in 24-48hrs; serum lipase is more sensitive and specific
- AXR: ?sentinel loop ?loss of psoas shadow
- CT abdo is the investigation of choice
- score using the Modified Glasgow criteria.
Modified Glasgow criteria (helpfully spells out 'pancreas'):
- Pa O2 <8
- Age >55
- Neurophils: WCC >15
- Calcium: <2
- Renal function: urea >16
- enzymes: LDH >600; AST >200
- Albumin: <32
- Sugars: glucose >10
Management of acute pancreatitis is:
- lots of IV fluid, catheter for fluid balance
- analgesia
- close observation
- treat cause
Complications of pancreatitis include:
- early
- sepsis
- shock
- ARDS
- renal failure
- DIC
- hypocalcaemia
- hyperglycaemia - 5% need insulin
- late
- necrosis and pseudocyst (=fluid in lesser sac)
- abscess
- fistulae
- chronic pancreatitis
Now for something completely different, visual field defects...
MRCP revision battle 27.5: Visual field defects
Visual fields pop up frequently in MRCP questions so it pays to learn this well!
The basic anatomy is illustrated below:
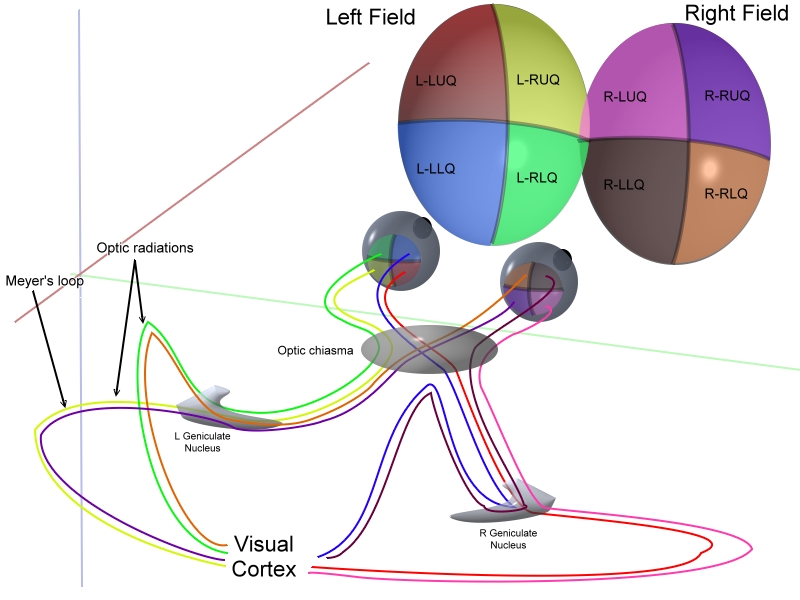
Armed this this anatomy lets look at the various patterns of field defect...
1: Bitemporal hemianopia

2: Homonymous quadrantanopia

3: Homonymous hemianopia

4: Central scotoma

5: Binasal hemianopia

Note that the fovea is supplied by both the PCA and MCA so may be spared in a PCA CVA.
In the calcarine sulcus peripheral regions are processed anteriorly while central regions are processed posteriorly.
Finally remember cortical blindness:
Wow, that was lots for one battle... lets move on to some urine for light relief...
The basic anatomy is illustrated below:
Armed this this anatomy lets look at the various patterns of field defect...
1: Bitemporal hemianopia
- caused by compression of the optic chiasm
- upper affected more than lower = due to pituitary tumour
- lower affected more than upper = due to craniopharyngioma
- I personally remember this as UP London City
2: Homonymous quadrantanopia

- superior homonymous quadrantanopia is a lesion in the temporal lobe
- inferior homonymous quadrantanopia is a lesion in the parietal lobe
- this can be remembered by thinking PITS - parietal inferior temporal superior
- if the defect is incongruous it is in the optic tract
- if the defect is congruous it is in the optic radiation/cortex
3: Homonymous hemianopia

- injury to the brain (eg bleed, tumour) on the opposite side to the field defect
4: Central scotoma

- usually caused by optic neuritis
5: Binasal hemianopia
- rare
- ?calcification of carotids
Note that the fovea is supplied by both the PCA and MCA so may be spared in a PCA CVA.
In the calcarine sulcus peripheral regions are processed anteriorly while central regions are processed posteriorly.
Finally remember cortical blindness:
- caused by bilateral occipital infarcts
- pupillary responses are preserved
- possibly small macular sparing
- patient may deny they have vision loss (=Anton's syndrome)
Wow, that was lots for one battle... lets move on to some urine for light relief...
MRCP revision battle 27.6: Paroxysmal nocturnal haemoglobinuria
Paroxysmal nocturnal haemoglobinuria is a condition in which blood cells are sensitive to complement-mediated lysis due to an inherited lack of surface glucosylphosphatidylinositol (GPI)
Features of paroxysmal nocturnal haemoglobinuria include:
Diagnosis is by urinary haemosiderin or + Ham's test (rarely done now)
Treatment is anticoagulation, transfusions when needed and possibly the smart new monoclonal antibody called eculizimab.
Now on to the last battle and some pretty pictures...
Features of paroxysmal nocturnal haemoglobinuria include:
- cola coloured/red urine in morning due to increase in RBC lysis overnight
- intravascular haemolysis
- pancytopenia
- thrombosis
Diagnosis is by urinary haemosiderin or + Ham's test (rarely done now)
Treatment is anticoagulation, transfusions when needed and possibly the smart new monoclonal antibody called eculizimab.
Now on to the last battle and some pretty pictures...
Subscribe to:
Posts (Atom)